Introduction
Oral malignant Melanoma is a rare malignancy representing 0.2% to 8% of all melanomas1 and 0.5% of all oral malignancies2-3. Although rare these tumors are known to have high potential for malignancy, invasiveness, and metastasis3-4, oral melanoma occurs slightly more often in males ( 2.8:1 male-to-female ratio ), and the age range is from 20 to 83 years with an average age of 56 years1,5. The clinical appearance of the tumor may be divided into following 5 types based on clinical features : pigmented nodular type, nonpigmented nodular type, pigmented macular type, pigmented mixed type, and nonpigmented mixed type6.
The clinical presentation of oral malignant melanoma varies from patient to patient. Almost one third of the patients are asymptomatic, observing just an irregular mass3. Masahiro Umeda et al described 3 growth phases of OMM : (1) a macular phase consisting of proliferation of dendritic melanocytes without apparent atypia and with simple hyperpigmentation in the basal cell layer and melanin incontinence; (2) a pigmented plaque phase consisting of preinvasive tumor cell nests in the lower epithelial layers; and (3) a nodular phase consisting of spindle-shaped or epithelloid tumor cells in the submucosa3.
A pigmented lesion of oral cavity should be viewed with suspicion since it does not possess clinical specificity. It must be differentiated from other forms of pigmented oral pathology including drug, disease or smoking associated melanosis, oral melanotic macule, Kaposi sarcoma, physiologic or racial pigmentations, melanocytic nevus and melanoacanthoma7. There is often a delay in diagnosis, and oral malignant melanoma is diagnosed after it has invaded deeper than average cutaneous melanoma8. Of the cases diagnosed as oral malignant melanoma 80% are present on the palate and maxillary gingivae, with remainder found on the mandibular gingivae, buccal mucosa, tongue and floor of the mouth9,10. Although melanomas in the oral cavity tend to be neglected as compared to skin, however a differential diagnose can be made clinically because of its red to black or brown color and irregular outline4,11. However need for histopathological confirmation after biopsy is highly recommended before diagnosis. Hereby, is a case of OMM in the left anterior mandibular gingiva.
Case Report
A 76 year old man presented to our department complaining of a painless gradually growing bluish black mass present in the left anterior region of the mouth since past 2 years (fig 1). Patient was a known hypertensive taking regular medication and gave no relevant medical history of any other systemic disease. Patient had no history of tobacco chewing and was non smoker but a regular drinker for more than 40 years.
 |
 |
Fig. 1
Clinical examination revealed a 2.5 X 1 cm irregular shaped bluish colored mass extending from distal aspect of left mandibular lateral incisor to distal aspect of second premolar. The lesion was non erythematous with ill defined borders and was soft on palpation. There was no significant regional lymphadenopathy and neck nodes were also negative. An intraoral periapical radiograph of the region along with a panoramic view and CT scan of the mandible were taken and evaluation revealed no bony involvement. Keeping in view the size of the lesion and recommendations of certain clinicians that incisional biopsy may promote metastasis14,15 an excisional biopsy was planned and performed under local anesthesia.
Fig. 2
Fig. 3
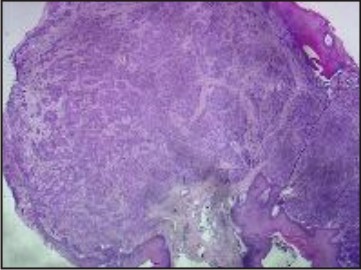
The tissue sample was divided into two parts and after proper labeling were send to two different laboratories. Both the pathology centers confirmed the diagnosis as malignant melanoma with histological findings showing melanocytes which were round to spindloid in shape with eosiniphilic cytoplasm, prominent eosinophilic nucleoli, pseudoinclusions, intra and extracellular melanin pigment in the malignant cells and stroma of the tumor. Pagetoid spread of the tumor in the epidermis in the form of single cells and nests of malignant cells was also present. Resection margins and the base in the biopsy sample were also infilterated with the tumor.
Fig. 4
Patient was advised immunohistochemical correlation with HMB45, Vimentin and S100 immunomarkers and a full body scan for metastasis to which he refused. Patient also refused any further treatment, but agreed for regular follow up once a month. There was a recurrence of the tumor in the same region approximately six month after the local excisional biopsy which the patient informed telephonically and refused to undergo any treatment for the same.
Discussion
Pigmentation of the oral mucosa is applied to various lesions or conditions featuring a change in tissue color. Two groups of pigmented lesions of the oral mucosa are recognized: 1) melanin associated lesions, including racial pigmentations, melanotic macules, melanotic nevi, and malignant melanoma ; and 2) nonmelanin associated associated lesions (e.e., blood-related pigmentations, metallic pigmentations7.
Primary mucosal melanomas of the oral cavity are very rare disease. Though skin melanomas have been clinically and pathologically classified and defined into various forms, a definitive classification of oral malignant melanoma is controversial14,16. In contrast to skin melanomas, etiologic factors of oral melanomas are not well established2,6,17, though factors such as tobacco use and formaldehyde exposure have been implicated[3], however Rapini et al1 claim that there is no proof linking the incidence of oral melanoma to the use of tobacco in any form rather surprisingly Kessides et al18 in their study have suggested the possibility that smoking may be inversely associated with melanoma risk. Mucosal melanomas have also been suggested to have more aggressive course than cutaneous melanomas and also poorer prognosis with a 5-year survival rate for oral melanomas between 0% to 20% 6,9,10,13,14,16,19,20,21. Oral mucosal melanoma may be primary or metastatic from other locations in the body2,9, therefore it is very important to rule out the possibility of a primary malignant melanotic lesion elsewhere in the body. Greene et al22 have described criteria for the diagnosis of a primary oral melanoma as 1) demonstration of clinical and microscopic tumor in the oral mucosa, 2) presence of junctional activity in the lesion, and 3) inability to show any other primary site. Oral melanomas may have certain clinical features that make it more suspicious for malignancy; like the lesional outline may be asymmetric, and the borders may be irregular due to lesion’s haphazard growth pattern. Most lesions are greater than 6mm in diameter at diagnosis. Another feature is color heterogeneity, with shades varying from brown to blue or purple to black or even red or white23.
Treatment of oral malignant melanoma include surgical resection with or without neck dissection, immunochemotherapy, and radiation therapy. Surgery is by far the most commonly used treatment moality5,8,9,13,19,20,21. Neck dissection in case of oral melanoma remains an issue of controversy. Some state that neck dissection should be performed only when palpable lymph nodes are present preoperatively8,9,13,14,19,20, while Catlin24 states that a neck dissection should be performed prophylactically, where there is a possibility of neck metastasis even in absence of palpable neck nodes. Role of radiotherapy as stated by most of the authors is only palliative and/or adjuvant as these lesions are believed to be poorly radiosensitive16,25,26, however slight regression without any significant increase in survival rates25. Chemotherapy have not been supported for intraoral malignant melanomas however they can be used for adjuvant and palliative purposes of therapy of metastatic melanoma20.
Umeda et al14 state that if adequate therapy was provided, the prognosis of oral melanoma have a better prognosis than reported previously. The treatment protocol they recommended is: 1) surgical resection of intraoral tumor; 2) neck dissection for clinically detected lymph nodes metastasis; 3) initiation of adjuvant immunochemotherapy with DTIC, ACNU, VCR, and OK-432 on the day of surgery; and 4) no biopsy because it might promote metastasis.
Conclusion
Oral malignant melanomas are rare but aggressive tumors with very low survival rates. Because of this all pigmented lesions in the oral cavity should be examined with suspicion. The treatment of choice for oral melanomas is wide surgical resection with or without neck dissection depending upon the state of lymph nodes with radio and chemotherapy as an adjuvant or palliative therapy. However recurrences and new lesions may occur, and close patient monitoring is imperative.
Review Of Literature
1. Rapini RP, Golitz LE, Greer RO, Krekorian EA, Poulson T : Primary malignant melanoma of the oral cavity: a review of 177 cases. Cancer 1985;55:1543-51.
2. Pliskin M: Malignant melanoma of the oral cavity : Human Malignant Melanoma. New York: Grune and Stratton, 1979, p 125-37
3. G.M. Gu, J.B. Epstein and T.H. Morton, Intraoral melanoma: Long-term follow up and implication for dental clinicians: A case report an literature review, Oral Surg Oral Med Oral Pathol Oral Endod 96 (2003), p. 404.
4. Mangabaro LAM, Hammond HL, Dalton MJ, et al: Oral melanoma: Case reports and review of the literature. Oral Surg Oral Med Oral Pathol 80:670, 1994.
5. Barker BF, Carpenter WM, Daniels TE, Kahn MA, Leider AS,Lozada-Nur F, et al. Oral mucosal melanomas: the WESTOP Banff workshop proceedings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:672-9.
6. Tanaka N, Mimura M, Ichinose S, et al: Malignant melanoma in the oral region: Ultrastructural and immunohistochemical studies. Med Electron Microsc 34:198, 2001.
7. M.Meleti, P.Vescovi, W.J. Mooi, Isaac van der Waal : Pigmented lesions of the oral mucosa and perioral tissues : a flow-chart for the diagnosis and some recommendations for management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 105: 606-16.
8. K.R. Magliocca, M.K. Rand, L.D.Su, J.I.Helman : Melanoma-in-situ of the oral cavity. Oral Oncology Extra (2006) 42, 46-48.
9. Rapidis AD, Apostolidis C, Vilos G, et al: Primary malignant melanoma of the oral
10. mucosa. J Oral Maxillofac Surg 61:1132, 2003
11. Midion Mapfumo Chidzonga, Leonard Mahomva,Clemence Marimo,Rudo Makunike-Mutasa: Primary Malignant Melanoma of the Oral Mucosa. J Oral Maxillofac Surg 65:1117-1120, 2007
12. Shou-Yen Kao, Jack Cheng-Chei Yang, Wing-Yin Li, Richard Che-Shoa Chang : Maxillary Amelanotic Melanoma: A Case Report. J Oral Maxillofac Surg 59:700-703, 2001
13. Gorsky M, Epstein JB. Melanoma arising from the mucosal surfaces of the head and neck. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:715-9
14. Umeda M, Shimada K. Primary malignant melanoma of the oral cavity—its histological classification and treatment. Br J Oral Maxillofac Surg 1994;32:39-47
15. Umeda M, Hideki Komatsubara, Takashi Shigeta, Yasutaka Ojima, Tsutomu Minamikawa, Yasuyuki Shibuya, Satoshi Yokoo and Takahide Komori : Treatment and prognosis of malignant melanoma of the oral cavity : preoperative surgical procedure increases risk of distant metastatis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:51-7
16. Austin JR, Byers RM, Brown WD, Wolf P. Influence of biopsy on the prognosis of cutaneous melanoma of the head and neck. Head Neck 1996;18:107-17
17. Paolo Garzino-Demo, Massimo Fasolis, Gian Marco La Terra Maggiore, Marco Pagano, Sid Berrone : Oral mucosal melanoma: a series of case reports. Journal of Cranio-Maxillofacial Surgery (2004) 32,251-257
18. Moore ES, Martin H: Melanoma of the upper respiratory tract and oral cavity. Cancer 8:1167, 1995
19. Maria C. Kessides, Lee Wheless, Judith Hoffman-Bolton, Sandra Clipp, Rhoda M. Alani and Antthony Alberg: Cigarette smoking and malignant melanoma: A case control study. J Am Acad Dermatol (2011) Volume 64, Issue 1, Pages 84-90
20. James E. Strauss and Sorrell I. Strauss: Oral Malignant Melanoma- A Case Report and Review of Literature. J Oral Maxillofac Surg 52:972-976; 1994
21. Thomas Mucke, Frank Holzle, Marco Kesting, Denys Loeffelbein, Luisa Robitzky, Bettina Hohlweg-Majert, Andrea Tannapfel, and Klaus-Dietrich Wolff: Tumor size and depth in primary malignant melanoma in the oral cavity influences survival. J Oral Maxillofac Surg 67:1409-1415, 2009
22. A.G. Smyth, R.P. Ward-Booth, B.S. Avery, E.W.H. To: Malignant melanoma of the oral cavity-an increasing clinical diagnosis? British Journal of Oral and Maxillofacial Surgery(1993)31, 230-235
23. Greene GW, Haynes JW, Dozier M, et al: Primary malignant melanoma of the oral mucosa. Oral Surg Oral Med Oral Pathol 6:1435, 1953
24. Spencer Kemp George Gallangher, Sadru Kabani, Robert Moskal; Persistent Melanoma In Situ: Case Report and Review. J Oral and Maxillofac Surg 66:1945-1948, 2008
25. Catlin D: Mucosal melanomas of the head and neck. AJR Am J Roentgenol 99:809, 1967
26. Marco Krengli, Laura Masini, Johannes Kaanders, Philippe Maingon, Swan Bing Oei, Abderrahim Zouhair, Enis Ozyar, Martine Roelandts, Maurizio Amichetti, Mathieu Bosset and Rene Mirimanoff : Radiotherapy in the treatment of mucosal melanoma of upper aerodigestive tract: Analysis of 74 cases. A rare cancer network study. Int J Radiation Oncology Biol Phys, Vol 65, No 3, 751-759, 2006
27. Fady B. Gera, K. Kian Ang : Radiation Therapy for Malignant Melanoma. Surgical Clinics of North America. Vol 76, No 6, December 1996 |