Introduction
With the advancement in all the spheres of medical profession, there has been most conspicuous and phenomenal progress in orthognathic surgery. The field of orthognathic surgery is not only fascinating but also challenging because it provides the patient an optimal aesthetic and functional result. However, best result can only be obtained, if the management of maxillo - mandibular deformities are meticulously assessed, planned and correctly executed from the very beginning. With the availability of numerous surgical procedures, it has become mandatory that there should be an organized pre-operative diagnosis and plan for achieving the most acceptable and perfect post –operative treatment results.
There are varieties of severe malocclusions that can be treated orthodontically but with a great deal of effort. Skeletal open bite is among the most challenging clinical situations that the orthodontists are facing orthodontists these days.1 Several treatment protocols have been proposed to correct anterior open bite malocclusions that can distinctly influence long term stability. Conventional orthodontic treatment is marked by significant open-bite relapse that is greater in non extraction treatment. So the patients with severe skeletal anterior open bite discrepancies can be managed with the use of a combined orthodontic and surgical treatment that includes segmental osteotomies of the anterior part of the maxilla. Clinicians have stopped performing open bite closure via mandibular surgery with counterclockwise rotation of the mandible and intermaxillary wire fixation because of the instability associated with this technique .Surgical management of anterior open bite can be achieved with various surgical techniques but most commonly maxillary impaction either alone or in conjunction with mandibular Osteotomy is used to eliminate open bites.2 Proffit et al in considering a hierarchy of stability for orthognathic surgery procedures, proposed maxillary impaction as the most stable procedure and maintained that the type of fixation (rigid internal or wire) in maxillary impactions did not influence stability.3 Bimaxillary procedures to correct anterior open bite appear to be less stable than maxillary procedures alone.4,5 Anterior segmental osteotomies are the procedures which can be accomplished intraorally without facial scar and do not require prolonged inter-maxillary fixation and there is no change in the posterior occlusion.6 These are not only stable but also versatile and can be undertaken for multiple deformities affecting the anterior portion of the jaw.
Case History
A 20 year old female patient came to the Department of orthodontics and dentofacial orthopedics, Himachal Dental College, Sundernagar, Distt Mandi (H.P) with a chief complaint of forwardly placed upper front teeth and inability to join front teeth.
After Clinical examination we found that it was a case of Angle class I malocclusion, anterior open bite- 1st premolar to 1st premolar (7mm), proclined maxillary and mandibular incisors, convex profile with average growth pattern. On cephalometric examination basal plane angle was increased, palatal plane was tipped up anteriorly and nasolabial angle was decreased.
Orthodontic Procedure:
After clinically examining the patient it was found that the overjet was not enough to surgically rotate the anterior maxillary segment clockwise by anterior maxillary Osteotomy and to push it posteriorly to reduce proclination of maxillary anterior teeth and to correct the open bite. Therefore both the lower first premolars were extracted and the anterior segment was retracted en mass with sliding mechanics to create over jet of 6mm.All the extraction spaces were closed in 8 months and the patient was ready for orthognathic surgery.
Surgical Procedure:
(Anterior maxillary Osteotomy -Cupar technique)7
The procedure was carried out under general anesthesia with nasal intubation, local infiltration with 2% lignocaine Hcl with adrenaline 1: 80000 as done in maxillary vestibule. Standard Cupar incision was given from first premolar to premolar .The Mucoperiosteum was elevated through this incision to expose the pyriform aperture & anterior wall of the maxilla up to the canine fossa. Upper first premolars were extracted on both the sides. Palatal tunneling was done from the extraction socket converging at midline. Keeping the gingivoperiosteal flap intact & well retracted vertical maxillary osteotomy was carried out from the socket of extracted premolars to pyriform aperture bilaterally followed by the palatal Osteotomy. After completing the Osteotomy, anterior maxillary segment was down fractured and Superior and posterior repositioning was done. Additional bone was removed from anterior segment or the adjacent maxilla. Suturing was done .No operative and postoperative complications were observed.
Post Surgical Orthodontics
Three months after surgical procedure it was found that approximately 1mm residual space was left distal to all canines, so post surgical orthodontics was performed for 3 months for residual space closure and minor leveling and alignment. Short class 2 elastics were given on both sides with class 1 elastics in the lower arch. The case was deboneded after 3 months of post surgical orthodontics.
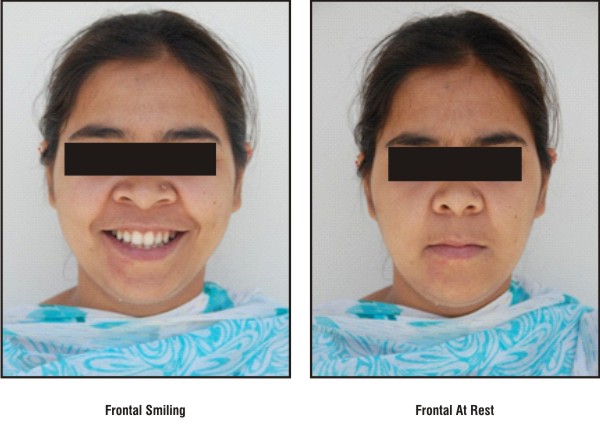
 | Pretreatment Photographs
 |
 | Posttreatment Photographs
|
 | Posttreatment Photographs
|
 | Pretreatment Radiographs
|
 | Post Treatment Radiograph
|
 | Radiographic Findings:
|
Discussion
Severe skeletal open-bite malocclusions are generally refractory to orthodontic means alone. The great amount of tooth extrusion is required to achieve inter arch incisor contact. The resistance to such extrusion offered by aberrant tongue and perioral muscle function, and the high potential for vertical relapse of extrusion that is achieved contribute collectively to the limited success of mechanotherapy8. A variety of operative techniques have been used and advocated for the correction of open-bite deformity. These include surgery in the anterior maxilla and mandible, posterior maxilla, simultaneous anterior and posterior maxilla, mandibular body, and ascending ramus. When the esthetic and functional requirements of the individual case can be satisfied by anterior maxillary surgery, this is the preferred operative approach since the surgical procedure is simple and the treatment results, including stability, are excellent. In most cases involving a Class II malocclusion, the posterior or combined simultaneous anterior and posterior maxillary Osteotomy is indicated. In cases with a Class III malocclusion, surgical intervention consisting of an anterior sub apical Osteotomy and chin reduction is advocated. So in this case report, as far as the esthetic and functional requirement of the case, patient of skeletal anterior open bite discrepancy was managed with the use of a combined orthodontic and surgical treatment that includes segmental Osteotomy of the anterior part of the maxilla.
The use of anterior maxillary Osteotomy for the correction of open bite, closed bite, underdeveloped maxilla, protruding maxilla was advocated by Mohnac. The procedure could be used concurrently with the mandibular correction of classII and class III malocclusions. According to Parnes (1966) the major advantage of surgical correction over the orthodontics was the “time factor”. The first report of an anterior segmental anterior maxillary osteotomy (ASMO) was published by COHN-Stock in 19219. After a transverse incision in the palatal mucosa, he made a wedge shaped ostectomy palatal to the anterior teeth. A greenstick fracture was then created at the ostectomy site, and the anterior maxilla was retracted. The anterior segment, however, relapsed within 4 weeks. Currently, mainly three variations of ASMO (Anterior segmental maxillary osteotomy) are used; the Wassmund, Wunderer, and down fracture methods. When the Wassmund method is used, the anterior maxillary segment derives its blood supply from both the facial and the palatal gingiva, as no flaps are raised. The planned Osteotomy sites are reached by tunneling under the mucoperiosteum10. The Wunderer method involves a palatal flap raised by means of a transverse incision of the palate. The anterior osteotomy is made after tunneling, leaving the buccal blood supply intact11 .In the down fracture method, on the other hand, a buccal flap is raised, and the palatal osteotomy is made after tunneling, leaving the palatal blood supply intact.
The usual indications for ASMO (Anterior segmental maxillary Osteotomy) are excessive vertical or antero-posterior development of the maxillary alveolar process in patients where the relationships between the posterior teeth are acceptable .When superior repositioning of anterior part of maxilla is the primary objective, the down fracture method (Cupar technique) is usually recommended, while the wunderer method is more practical for posterior repositioning. The main advantage of Wassmund method is the excellent postoperative blood supply, and this technique is recommended by some authors for all cases other than those requiring superior repositioning. We corrected maxillary prognathism with anterior maxillary Osteotomy (Cupar technique). No operative and postoperative complications were encountered.
References:
1. Lisen Espeland, Paul A. Dowling, Karim A. Mobarak, and Arild stenvik- Three year stability of open-bite correction by1-piece maxillary osteotomy .Am J Orthod Dentofacial Orthop 2008;134:60-6.
2. Lew KK- A ten year follow up case report follow surgical correction of anterior open bite. Aust. Dental journal 1991,36; 109-112.
3. Profitt.W.R.L.J, Bailey et al: A long term stability of surgical open bite correction by Le Fort 1 osteotomy. Angle orthodontics 2000; vol 36: 110-12
4. Arpornmaeklong P, Heggie AA: Anterior open-bite malocclusion: Stability of maxillary repositioning using rigid internal Fixation. Aust Orthod J 2000;16:69-81.
5. Hoppenreijs , Freihofer , Stoelinga , Tuinzing ,Van’t H, van der Linden et al : Skeletal and Dento-alveolar stability of Le Fort I intrusion osteotomies and Bimaxillary osteotomies in anterior open bite deformities. A Retrospective three-centre study. Int J Oral Maxillofac Surg 1997;26:161-75.
6. Bell.W.H.: Lefort 1 ostotomy for the correction of maxillary deformities . Journal of oral surgery 33:412; 1975.
7. Cupar, I. : Die Chirurgische Behandlung der Form-turd Stellung-Sveranderungen Des Oberkiefers, O&err. Z. Stomatol. 51: 565, 1954; Bull. SC. Cons. Acad. R..P.F. Yougosl.2: 60, 1955.
8. R.William McNiell: Surgical orthodontic correction of open -Bite malocclusion .Am J Orthod Dentofacial Orthop 1973;64; 108-11.
9. Cohn-Stock, G.: Die Chirurgische Immediatre-Gulierung der Kiefer, Speziell die chirorgiscle Behandlung der progmataie, Vjschr, Zahnheilkd. 37: 320-329, 1921.
10. Wassmund, M.: Lehrbueh der praktischen Chirurgie des Mundcs und der kicfer, Leipzig, 1935, Hermann Meusser, vol. 1.
11. Wunderer, S.: Die Prognathie Operation Mittels Frontal Gestieltem Maxillafeagment, Osterr. Z. Stomatol. 59: 98, 1962.
12. Epker.B.N: A modified anterior maxillary osteotomy. J Max-Fac Surg ,1977: 5; 35-8. |


