|
|
|
| Technique Clinic - A New Method For Bonding Lingual Retainer |
Vishal Seth 1 , Prasanth Kamath 2 , Venkatesh M. J. 3
1 Senior Lecturer, Department of Orthodontics - HDC, SunderNagar
2 Professor And Head Of Department, Department of Orthodontics, - Syamala Reddy Dental College, Marathalli, Munekolala, Bangalore - 560037
3 Professor, Department of Orthodontics - Syamala Reddy Dental College, Marathalli, Munekolala, Bangalore - 560037
|
| Address For Correspondence |
Dr. Vishal Seth
Senior Lecturer,
Department of Orthodontics,
Himachal Dental College, Sundernagar HP
Email: drvishal13@rediffmail.com,
Mobile No: 9986514414 |
| Abstract |
| Since the beginning of the century, fixed retainers, have been recommended after correction of rotated or tipped incisors and for maintenance of increased intercanine width. The importance of a passive and precise positioning has been stressed because tension in the wire will result in a failure of retention. Since the introduction of bonding in orthodontics, fixed retainers have steadily grown in popularity among orthodontists. They have the advantage of being fixed, esthetic, unobtrusive and provide stability of treatment results without much patient cooperation. However the accurate placement of lingual retainers has been questioned in the past, which has led to the development of numerous direct and indirect techniques for the precise placement of bonded retainers. |
|
| Keywords |
| Lingual, Retainer, Bonded, Relapse. |
|
| Full Text |
Introduction
In the late 1970s and early 1980, Zachrisson1-4 published several papers elucidating the application of bonded lingual retainers. Since then, the use of lingual retainers has steadily grown, and several methods for delivering fixed lingual retainers have been introduced. Following the introduction of the acid etch technique, a variety of methods have been suggested for fabrication and bonding of fixed retainers to the lingual surface of lower canines or to the lingual surface of all lower anterior teeth8However, the accurate and passive placement of the retainer has always been a matter of concern. Elastics2, dental floss 10 or ligature wires help in securing the retainer in place but cannot ‘precisely’ position the retainer. Holding the retainer wire with a plier or finger pressure is especially risky1, as any movement during curing can weaken the bond. A silicone transfer tray is time-consuming to fabricate and trim11, and can become deformed during the bonding procedure. Vacuum-formed locating splints provide accurate positioning, but require an indirect technique and additional chair time for removal of excess composite6. The aim of this study is to described the use of molar bands for precise and passive placement of bonded lingual retainers.The bands can be likened to a set of transfer trays for holding and placing the retainer at its predefined position.
Material and method :
The molar bands are removed and subsequently reseated loosely without cementation (Fig 1 & 2).
 | Figure 1: Before Debonding
 |
 | Figure 2: Molar Bands Being Removed
|
Alginate impressions are made using standard trays, . the bands are removed and placed at the appropriate position in the impression ( Fig 3) (Sticky wax can be used for reinforcing the position of the bands). Accurate casts are poured with dental stone ( Fig 4 ). The position of the retainer is marked by the orthodontist on the cast, and accordingly a precisely fitting retainer is adapted by using 0.0155-inch multi- stranded wire ( Fig 5 )(3M/Unitek). The terminal ends of the retainer end up in close configuration with the molar bands. The retainer is secured on the working cast with Super Glue (quickfix) and the terminal ends of the retainer are soldered to the molar bands ( Fig 6 & 7 ). The molar bands are now carefully removed from the working cast along with the retainer and placed back in the patient’s mouth. The teeth are dried and etched, and bonded with light- cured adhesive (Transbond XT System) ( Fig 8 ). After bonding, with the help of a high-speed tungsten carbide bur, the retainer is cut distal to the last bonded tooth on either side ( Fig 9 ). The excess composite is trimmed and smoothened. ( Fig 10 )
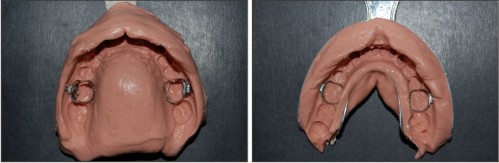 | Figure 3: Alginate Impressions With Molar Bands In Place
|
 | Figure 4: Cast After Pouring
|
 | Figure 5: 0.0155-inch Multistranded Wire Bent To End Up In Close Configuration With The Molar Bands
|
 | Figure 6: Retainer After Soldering To The Bands
|
 | Figure 7: Retainer Seated In Patient’s Mouth
|
 | Figure 7: Molar Bands Along With The Soldered Retainer Wire
|
 | Figure 8: Curing Of Retainer
|
 | Figure 9: Retainer Cut Distal To The Last Bonded Tooth
|
 | Figure 10: Finished Lingual Retainer
|
Discussion
The technique described eliminates the difficulties en- countered in direct bonding of a lingual retainer, which can be especially challenging in patients with upright mandibular incisors. According to Zachrisson13, the primary causes of fixed retainer bond failure can be attributed to: 1. some degree of distortion during setting of adhesive; 2. use of too little adhesive; 3. direct trauma to the retainer. Abrasion of composite was also implicated as the primary reason for bond failure in a study by Artun and Orbye12, where most of the patients had deep overbites after orthodontic tooth movement. For these reasons, bonded retention of maxillary anterior teeth has remained difficult and has not gained wide acceptance. However, the present method of placing the retainer makes accurate placement possible,even in situations where it could not easily be considered before, as defined above.As the bands sit firmly on the molars,good adaptation of the wire on the lingual side is achieved. The placement is positive, exact and firm, which enables the operator to work freely with both hands, confident that the unit will not dislodge during manipulation of the composite adhesive material. The wire itself is in its passive, unstressed state. Thus, the setting of adhesive is totally undisturbed. However, one disadvantage of this technique is a brief increase in the laboratory time for retainer fabrication and soldering.
Conclusion
Retention is a necessary stage of the successful long-term management of most orthodontic patients. Precision in fabrication, accuracy during placement on the teeth, and avoidance of any irritation to the gingiva are necessary requirements for a lingual fixed retention. The method described in this article seems to fulfill all of these prerequisites and gives significant chairtime advantages. It can be used for the fabrication of any kind of lingual fixed retainer and for periodontal splinting of the teeth. Different sizes and qualities of wires can be incorporated, depending on the indications of the particular case and the clinician's consideration. The method described in this report seems to fulfil all these prerequisites. Overall, molar bands appear to serve as efficient transfer mechanisms for accurate and stable placement of the retainer, simplifying and streamlining the procedure to such an extent that 15 minutes is more than enough to bond the retainer in place.
References
1. Zachrisson BU. Clinical experience with direct-bonded orthodontic retainers. Am J Orthod 1977; 71: 440–48.
2. Zachrisson BU. The bonded lingual retainer and multiple spacing of anterior teeth. J Clin Orthod 1983; 17: 838–44.
3. Zachrisson BU. Bonding in orthodontics. In: Graber TM, Swain BF (Eds). Orthodontics: Current Principles and Techniques. St Louis: Mosby, 1985: 485–563.
4. Zachrisson BU. Adult retention: a new approach. In: Graber LW (Ed.). Orthodontics: State of the Art; Essence of the Science. St Louis: Mosby, 1986: 310–27.
5. Cerny R. Permanent fixed lingual retention. J Clin Orthod 2001; 35: 728–32.
6. Corti AF. An indirect-bonded lingual retainer. J Clin Orthod 1991; 25: 631–32.
7. Hayadar B, Hayadar S. An indirect method for bonding lingual retainers. J Clin Orthod 2001; 35: 608–10.
8. Bantleon HP, Droschl H. A precise and time-saving method of setting up an indirectly bonded retainer. Am J Orthod Dentofacial Orthop 1988; 93: 78–82.
9. Hobson RS, Eastaugh DP. Silicone putty splint for rapid placement of direct-bonded retainers. J Clin Orthod 1993; 27: 536–37.
10. Meyers CE, Vogel S. Stabilization of retainer wire for direct bonding. J Clin Orthod 1982; 16: 412.
11. Lubit EC. The bonded lingual retainer. J Clin Orthod 1979; 13: 311–13.
12. Artun J, Urbye KS. The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium, Am J Orthod 1988; 93: 143–48.
13. Molar bands for precision bonding of lingual retainers – journal of orthodontics vol. 34, 2007 ,12- 15 |
|
|
|
|
|
|