Introduction:
Reported estimates suggest that about one out of every four persons under the age of 18 sustains a traumatic dental injury in the form of an anterior crown fracture1.Coronal fractures of permanent incisors represent 18-22% of all trauma to dental hard tissues, 28-44% being simple (enamel +dentin) and 11-15%, complex (enamel +dentin +pulp). Of these 96% involve maxillary central incisors. 2 Owing to the high incidence of dental trauma, dentists are confronted with managing and restoring fractured teeth on a regular basis. Hence, techniques that restore aesthetics, and improve long-term success rates are of potential value and should be considered. Reattachment of fracture fragment with or without reflection of surgical flap is one such procedure. The first published case reattaching a fractured incisor fragment was reported in 1964 by Chosack and Eidelman.3 At present, the literature reports vast numbers of such cases, with successful outcomes.
Although the type and location of fracture depends upon age of patient, amount of force and direction of blow4; an in vitro investigation by Stokes5 concluded that most of the traumatised incisors fracture in an oblique fashion from the labial to lingual aspects with the fracture line proceeding in an apical direction. Oblique coronal fractures that involve pulp and extend apically into the root (subgingival) may also invade the critical area of biologic width. These fractures are particularly challenging and require elevation of a periodontal flap for surgical correction of biologic width and for gaining access to the fractured site for reattachment.
This case report highlights the surgical reattachment of a case of complicated crown-root fracture in maxillary central incisor using intraradicular support in the form of an endodontic post.
Case Report:
A 21-year-old male patient reported to the dental hospital with a fractured maxillary central
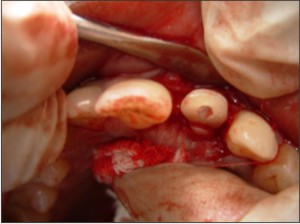
incisor. History revealed trauma seven days back, medical history was non-contributory. There was no other injury associated with the soft tissues or alveolar bone. Intra-oral clinical and radiographic examination revealed a complicated crown-root fracture (involving pulp) of maxillary left central incisor (Figures 1, 2). The fracture line was oblique extending in apical direction from labial to palatal surface. Upon probing, it was found that the biologic width was being encroached on the palatal aspect. The fractured fragment was loosely attached to the root. Various available treatment options were explained to the patient, out of which he preferred reattachment of the fractured fragment.
 | Fig. 1: Pre Operative View Showing Complicated Crown-root Fracture Of Maxillary Left Central Incisor
 |
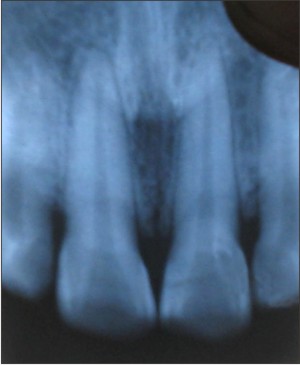 | Fig. 2: Preoperative Radiograph Shows The Fracture Line
|
Under local anaesthesia, the fractured fragment was removed atraumatically and stored in distilled water to be used at a later stage. The adaptation of the fragment to the underlying root was checked. Single sitting root canal treatment was completed under rubber dam and the post space was prepared to receive a prefabricated parallel sided stainless steel post (Parapost Coltene. Whaledent, Mahwah, NJ). The fractured fragment was removed from the distilled water, pulpal remnants were removed and it was tried on the cut end of the post. A groove was made on the fractured fragment (Figure 3)
 | Fig. 3: Groove Prepared In The Fractured Fragment.
|
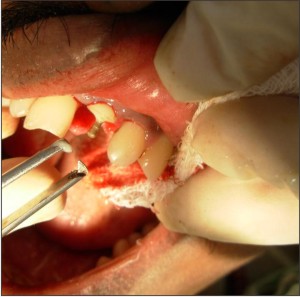
and its adaptation to the underlying post restored root was checked. Once the desired fit was confirmed, it was again stored in distilled water. Full thickness surgical flap was elevated to gain access to the apical extension of the fracture (Figure 4).
 | Fig. 4: Surgical Exposure Of The Fractured Site.
|
Biologic width was restituted by performing osteoplasty on palatal aspect. The post was cemented with the help of dual-cure Rely X U100 self adhesive universal resin cement (3M ESPE, St. Paul, Germany) (Figure 5). Any excess cement was removed as it could have altered the fit of the fragment. It was then light cured (QHL75 Curing Light, Dentsply, Addlestone, Surrey) for 20 sec. Groove in the fractured fragment was filled with the same cement and the fragment was repositioned correctly and cured for 20 seconds each from palatal, labial and incisal surfaces. The surgical flap was secured in place with the help of sutures (Figure 6), which were removed after one week. Occlusion was checked and post operative instructions were given to the patient.
 | Fig. 5: Luting Of The Post With Dual-cure Rely X Cement
|
 | Fig. 6: Reattachment Of The Fragment Followed By Sutures
|
Clinical and radiographic examinations carried out after 1 month, 3 months, 6 months and 1year confirmed the satisfactory esthetic and functional outcome of the treatment with no associated endodontic or periodontal problem. Radiographic examination after 1 year revealed satisfactory osseous healing (Figure 7).
 | Fig. 7: Follow Up Radiograph At One Year
|
Discussion:
Anterior tooth fracture poses immense distress for the young patient. But, preservation of natural tooth structure definitely provokes a positive emotional and social response from the patient.6 Due to the advent of advanced composite resin cements; reattachment has gained new dimensions in recent years. However, this technique can be used only when the intact tooth fragment is available.7 This case report presents a case of complicated crown-root fracture successfully managed by reattachment of the fractured fragment after performing endodontic therapy.
Rely X U100 self-adhesive universal resin cement (3 M, ESPE) was used for luting the post as this cement allows a single step luting process thereby eliminating any procedural technique sensitivity and also does not require any surface pre-treatment of the substrate such as, silanation or etching and bonding.8 This simplified the reattachment procedure.
The clinical importance of an intact biologic width is in the maintenance of periodontal health. Once the biologic width gets compromised due to fracture, surgical correction must be performed to restitute the invaded area.9 In this case, fracture line invaded the biologic width on the palatal aspect but this was restricted to a small area and was still supraosseous. Hence it was decided to reflect surgical flap and perform osteotomy of the localized area. The excellent healing achieved in this case supports the success of surgical reattachment procedure.
Reattachment of the original tooth fragment poses many advantages over other restorative methods because the tooth colour, contour, texture, incisal translucency and occlusal contacts remain the same.9-11 Moreover, reattached fragment may sometimes act as a transitional restoration if a definitive prosthetic restoration, such as crown is required.12 These advantages of reattachment and high success rates negate the use of other expensive restorations.13 But this single visit, multidisciplinary approach to crown root fracture requires consideration of periodontal, endodontic, restorative and occlusal factors. Follow-up is of critical importance in such cases. The patient should be followed regularly for a few years. During each follow-up visit, the clinician should confirm the Esthetics, tooth mobility and periodontal status of the reattached tooth.
Conclusion
This paper describes a successful clinical technique for management of an oblique crown-root fracture of a maxillary central incisor. Use of single step resin cement simplified the procedure of surgical reattachment. However, this approach should be reserved for those patients who demonstrate adequate plaque control with low risk of periodontal disease.
References:
1. Andreasen JO, Ravn JJ. Epidemiology of traumatic dental injury to primary and permanent teeth in a Danish population sample. Int J Oral Surg 1972; 1:235–9.
2. Pagliarini A, Rubini R, Rea M, Campese M. Crown fractures: Effectiveness of current enamel dentin adhesives in reattachment of fractured fragments. Quintessence Int 2000; 31:133-6.
3. Chosack A, Eidelman E. Rehabilitation of a fractured incisor using the patient's natural crown — case report. J Dent Child 1964; 71: 19–21.
4. Andreasen JO. Etiology and pathogenesis of traumatic dental injuries: a clinical study of 1.298 cases. Scand J Dent Res 1970; 78:329.
5. Stokes A, Hood J. Impact fracture characteristics of intact and crowned human central incisors. J Oral Rehabil 1993; 20: 89–95.
6. Baratieri L.N., Monteiro S.: Tooth fracture reattachment: Case reports. Quint Int 1990; 21: 261 - 270.
7. Simonsen R.J.: Traumatic fracture restorations: An alternative use of the acid etch technique. Quint Int. 1979; 10: 15 - 22.
8. Ceballos L, Garrido MA, Fuentes V, Rodriguez J. Mechanical characterization of resin cements used for luting fiber posts by nanoindentation. Dent Mater 2007; 23: 100-105.
9. Baratieri LN, Ritter AV, Monteiro Ju´ nior S, de Mello Filho JC. Tooth fragment reattachment: an alternative for restoration of fractured anterior teeth. Pract Periodontics Aesthet Dent 1998; 10:115–25.
10. Reis A, Loguercio AD, Kraul A, Matson E. Reattachment of fractured teeth: a review of literature regarding techniques and materials. Oper Dent 2004; 29:226–33.
11. Reis A, Loguercio AD. Tooth fragment reattachment: current treatment concepts. Pract Periodontics Aesthet Dent 2004; 16:739–40.
12. Maia EAV, Baratieri LN, de Andrada MAC, Monteiro S. Jr, de Araujo EM. Jr. Tooth fragment reattachment: Fundamentals of the technique and two case reports. Quintessence Int 2003; 34:99-107
13. Wadhwani CPK. A single visit, multidisciplinary approach to the management of traumatic tooth crown fracture. Br Dent J 2000; 188:593-8. |