INTRODUCTION
As rightly said, “BEAUTY LIES IN THE EYES OF THE BEHOLDER”An acceptable cosmetic effect in any dental restoration has always been regarded as important to good dentistry. A well-made prosthesis will fail if it is deficient in this respect.Aesthetics includes the appreciation and response to the beautiful in art and nature. Aesthetics has been given many definitions in dentistry but according to Young. “It is apparent that beauty, harmony, naturalness and individuality are major qualities” of aesthetics. The dentist must visualize aesthetics in relation to the patient and then translate that visualization into an acceptable aesthetic result. The success of his efforts depends upon his artistic ability, his powers of observation and his experience.
Modern dentistry aims at conservation of remaining tooth structure. Recently dental researchers have attempted to incorporate fiber reinforcement technology into dental laboratory procedures and to add fibers to dental resins. Restoration of a root canal-treated tooth because of a significant loss of structure is achieved with a post and a core. New, prefabricated posts have been introduced for post-and-core endodontic restorations. They are manufactured from special fibers reinforced with ceramic and composite. The main advantage of this new biocompatible metal-free post is that it enables reconstruction of the destroyed tooth structure to its natural aesthetics. The objective of this case report is to describe the Prostho-endo procedures for post-and-core system preparation using a fiber-rein-forced post and metal-free crowns over it which is depicted by fine clinical skills.
CASE REPORT:
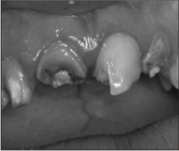
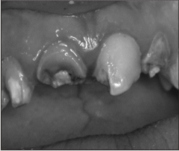
A 35 year old patient reported in Department of Prosthodontics, Dasmesh Institute of Research and Dental Sciences , Faridkot , Punjab with Anterior teeth restored with faulty Prosthesis (Acrylic Bridge). Intra oral examination revealed maxillary incisors restored with a prosthesis which was not acceptable aesthetically(Fig-1,2).
 | Fig 1
 |
 | Fig 2
|
She had not smiled all these years because of faulty discolored artificial looking acrylic bridge on her teeth.Keeping patients need in mind the treatment plan for the patient involved fiber post and core fabrication followed by all ceramic crowns [IPS e-max] cementation with 12,11,21,22.
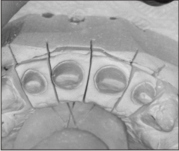
Two-thirds of the total canal length was used for the post hole. A reamer of low-speed hand piece was applied along the entire length. A proper-sized Fiber Post was selected according to canal thickness and then cut at the required length. The post was adjusted into the canal. The preferred adhesive technique is dual-cure resin cementation [Calibra Esthetic Resin Cement, Dentsply] of the post and the composite core construction because of the similarity of the physical properties of metal-free posts and ceramic composite cores to those of dentin. The working field was isolated. The root canal surface was etched with 37% phosphoric acid solution for 15 seconds, rinsed thoroughly, and dried with paper points. Equal parts of dual-curing, Hydrophilic Bond and Activator were mixed and applied into the root canal with an endodontic instrument. A thin, uniform coat of bonding resin was applied over the post. Equal parts of translucent [allows maximum light transmission] shade, Base paste and Catalyst of the dual-cure resin cement were mixed and was spread on the surface of the fiber post and then into the post preparation with lentulo spiral. Each post was cemented separately one by one. The post was carefully seated immediately, a 10 second light exposure “pre-cure” of excess cement was done and the “gel” cement was removed with the help of blunt instrument. The post was stabilized for approximately 6 minutes from the beginning of the mixing for the self cure to set. Once the posts were stabilized, all the accessible areas of the post for 20 seconds each, were light cured with visible light curing unit (470nm) (Fig-3). Additionally the gaps between the core and the tooth structure were filled with a core build-up material. (Fig-4)
 | Fig 3
|
 | Fig 4
|
The tooth restored with a post-and-core system was then prepared for the planned all-ceramic restoration. .The color of the definitive restorations was already defined. After the core was built up and teeth preparations, gingival retraction was done with #00 size [Ultra Dent Product, Utah, USA] ; impression was made with polyvinyl siloxane [Aquasil , Dentsply Caulk ]. Provisional restoration was fabricated and luted using eugenol-free zinc oxide cement [Rely X Temp NE, 3M ESPE]. All ceramic crowns were fabricated in the laboratory [IPS e.max [Ivoclar/ Vivadent] (Fig-5,6)
 | Fig 5
|
 | Fig 6
|
Once the marginal integrity , fit, occlusion and esthetics were verified . The internal surface of the all-ceramic restoration was etched with buffered hydrofluoric acid, washed and dried. Then Calibra Saline coupling agent was applied to the etched clean internal surface for30 seconds and rinsed thoroughly for 20 seconds. Air dried with dental air syringe.
The cores built up surfaces were etched with 37% phosphoric acid solution for 15 s, rinsed thoroughly. Equal parts of dual-curing, Hydrophilic Bond and Activator were mixed and applied into the core surfaces. A thin, uniform coat of bonding resin was applied onto the internal surface of crowns. Equal parts of selected shade Base paste and Catalyst of the dual-cure resin cement [Calibra esthetic resin cement, Dentsply] were mixed and then layered uniformly onto the internal surface of crowns. The crowns were seated one by one with gradual and rocking motion gentle pressure to ensure optimal seating. A 10 second light exposure “pre-cure” of excess cement was done and the “gel” cement was removed with the help of blunt instrument. Then light cured for 20 seconds each from the buccal, lingual and interproximal aspects. The occlusion was checked and a final polish was achieved. Patient was instructed to continue with the oral hygiene regime. (Fig.7a,7b).
 | Fig 7A
|
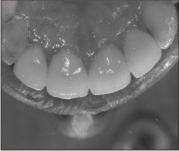 | Fig 7B
|
Pre operative and post operative photographs reveal marked improvement in aesthetics of patient (Fig.8, 9).
 | Fig 8
|
 | Fig 9
|
DISCUSSION
David F. Levine stated that improper management of the periodontal tissues during restorative procedures is a common, but often overlooked, cause of failure. When a restoration is placed, the preservation of an intact, healthy periodontium is necessary to maintain the tooth or teeth being restored. Predictable long-term restorative success requires a combination of restorative principles with the correct management of the periodontal tissues2.
Clinical observation reveals a series of advantages for the metal-free restorations. This technique is easy to perform and safe for both patient and dentist and are highly aesthetic. Cast posts and cores are commonly used because of their superior mechanical properties. However, if a ceramic crown is chosen as the final restoration, the color and opacity of the post may lead to discoloration and shadowing on the gingival and cervical areas of the tooth. A cast post can cause early root fracture due to the excessive tooth structure removal and direct transmission of masticatory loading forces from the post on the tooth root. There may be as high as a 100% incidence of root fracture in teeth restored with a cast post and core3. The rate of root fracture for teeth restored with a post and core is 50% for stainless-steel posts and 0% for the carbon fiber post (C-Post) group4. To solve this esthetic problem, tooth colored fiber post systems were introduced; these are capable of resisting occlusal loads and have light transmission characteristics similar to those of natural teeth.5
The union of the luting composite cement of the metal-free post and dentin yields a stable and homogeneous, newly created structure whose aesthetics and durability is remarkable. The fiber-reinforced post-and-core system together with adhesive cementation procedure is easy and safe to use in clinical practice. It ensures high-quality aesthetics and the durability of the metal-free restorations.
CONCLUSION
According to the obtained results by this prostho-endo endeavor it can be very well appreciated that comprehensive treatment approach requires multidisciplinary team work for successful rehabilitation leading to conservation of the tooth and its permanent restoration with excellent aesthetic. In this case report an attempt was made not only to rehabilitate destroyed tooth structure of oral cavity but also to rejuvenate facial aesthetics and smile which provides confidence, solace and comfort to the patient.
REFERENCES
1. Friedler AP, Leinfelder K. The clinical application of a new post. Dent Today 1999;18:84–5.
2. David F. Levine, Mark Handelsman and Nicolas A. Ravon “Crown Lengthening Surgery: A Restorative Driven Periodontal Procedure” Journal of the California Dental Association 1999.
3. Isidor F, Brondum K. Intermittent loading of teeth with tapered, individ-ual cast or prefabricated parallel-sided posts. Int J Prosthodont 1992;5:257–61.
4. Dean JP, Jeansonne BL, Sarkar N. In vitro evaluation of a carbon fiber post. J Endodon 1998;24:807–10.
5. Isidor F, Odman P, Brondum K. Intermittent loading of teeth restored using prefabricated carbon fiber posts. Int J Prosthodont 1996;9:131–6. |