INTRODUCTION
Uncontrolled mineralization due to failure of enzyme, pyrophosphatase, reduced capillary permeability and reduced blood supply leads to calcifications.
.Root canal in teeth in which calcific deposits have blocked access to the canal (s), treatment efforts are often thwarted.1 An effort to locate the residual canal may remove large amounts of dentin and there is a risk of perforating or fracturing the root. 1
CALCIFICATION OF THE PULP CAN OCCUR DUE TO
1. Mineralization in response to various irritants
2. Aging.
TUBULAR / DENTINAL SCLEROSIS
Milder or moderately irritating agents produce tubular sclerosis. It is a condition of the primary dentinal tubules where they are ultimately occluded.2 Sclerotic dentin, on the other hand, may be considered a defense mechanism of the pulp dentinal complex because its formation alters the permeability of the tubules, blocking the access of irritants to the pulp.2,3 Certain drugs such as calcium hydroxide and corticosteroids, when placed on the dentin after cavity preparation have also been demonstrated by studies to cause sclerosis. Apparently, some remineralisation also occurs when sedative dressings, such as zinc oxide eugenol, are placed in carious cavities.2
SECONDARY DENTIN
Continuous deposition of the dentin, which tends to reduce the volume of the pulp takes place throughout life. Schour has claimed that 4 microns of secondary dentin is deposited daily. The deposition of dentin is slow and gradual but does increase after the age of 35-40 years. There is no firm evidence that systemic conditions such as arteriosclerosis leads to a higher incidence in pulpal calcifications.4In molars, deposition is seen greatest on the pulpal floor, to a lesser extent on the roof, and least on the side- walls. Therefore, with age, pulp chambers decrease significantly in height i.e. in occlusoradicular direction but not extensively in width i.e. in mesiodistal direction.5,2 As a result, the horns of the pulp in molars are often left behind. They also recede, but not as much as the rest of the pulp tissue.2 In upper anterior teeth, the greatest dentin deposition occurs on the lingual wall of the pulp chambers, as a result of masticating forces with subsequent deposition in the incisal tip and floor of the pulp chamber.
REPARATIVE DENTIN
Localized secondary dentin laid down in areas of focal injury in response to various irritants is more haphazardly organized and is termed as reparative secondary (irregular, irritation or tertiary) dentin.6 In humans, the average rate of reparative dentin formation has been reported to be 2.8 microns for deciduous teeth and 1.5 microns for permanent teeth. Operations on the dentin, with resultant damage to the involved odontoblasts, cause temporary derangement in mineralization shown by the formation of a basophilic line. This has been termed as a calciotraumatic reaction. The presence of abundant amounts of reparative dentin does not appear to be correlated with pulp- test readings.2
RETROGRESSIVE PULP CHANGES
These altered pulp conditions are
1. Atrophy and fibrosis
2. Dystrophic calcification (calcific metamorphosis )6
P.E. Lovdahl and J.L. Gutmann have summarized pulpal responses to irritation as follows7:
1. Rapid death with canal patency.
2. Irritational response with pulpal demise
3. Extensive irritational response and pulp system exposure
CALCIFICATIONS OF PULP
. The classification by Kronfield is most commonly used.4
1. Discrete pulp stones (denticles, pulp nodules )
2. Diffuse calcification.
According to Seltzer, denticles may be classified as
a. According to structure – true or false.
The difference between the two is morphologic, not chemical
b. According to size -fine, diffuse mineralizations (also called fibrillar mineralization) and denticles.
c. According to location – embedded or interstitial, adherent and free denticles.
CALCIFIC METAMORPHOSIS
Calcific metamorphosis is defined as a pulpal response to trauma that is characterized by deposition of hard tissue within the root canal space and is commonly found in young adults in the anterior region of the mouth.8
TREATMENT PLANNING
It should be monitored radiographically and treated only if an area of rarefaction or clinical symptoms develop. 9
Radiographs -Reducing the kVp and increasing the milliamperage accordingly increases the contrast and may make film interpretation easier.
Multiple preoperative views may help the clinician locate root canals or establish the presence of additional root or canals.
The use of buccal object rule and radiographic markers such as cotton pellet- stabilized burs/ segments of foil/ gutta percha can help determine the bucco- lingual orientation in posterior teeth. However, to help determine the labio- lingual position during the non- surgical treatment of calcified canals in anterior teeth one is usually forced to rely more on the visual aspect.
With magnification, a world of remarkable lucid detail within the tooth becomes available, facilitating considerably more accurate,thus more conservative ,penetration through dentin.10
MANAGEMENT
NONSURGICAL MANAGEMENT
ORIFICE RECOGNITION
An important fact to remember is that the canal space in normal root canal anatomy is always in the cross- sectional center of the root. Similarly the pulp chamber is (or was, before calcification) located in the cross sectional center of the crown.11In a tooth with a calcified pulp chamber, the distance from the occlusal surface to the projected pulp chamber is measured from the preoperative periradicular film, or preferably from a bite- wing film, which maximizes accuracy. They applied the buccal object rule for the determination of calcified root canals as follows:
After the initial access opening, the bur is left in place and three radiographs are taken:
1. Straight – on to the bucco- lingual dimension to determine the position of the head of the bur in the root canal in the mesio- distal dimensio
2.Radiograph taken with a 20 o horizontal angulation with the cone shifted distally.
3. Radiograph taken with a 20 o horizontal angulation with the cone directed mesially.
The last two radiographs give information regarding the relation of the bur to the canal lumen in the bucco- lingual dimension.12
Krasner and Rankow have given certain laws which are particularly useful in locating calcified canal orifices. These are:
1. Law of symmetry 1: Except for maxillary molars, the orifices of the canal are equidistant from a line drawn in a mesiodistal direction through the pulp- chamber floor.
2. Law of symmetry 2: Except for maxillary molars, the orifices of the canals lie on a line perpendicular to a line drawn in a mesiodistal direction across the center of the floor of the pulp chamber.
3. Law of color change: The color of the pulp chamber is always darker than the walls.
4. Law of orifices location 1: The orifices of the root canals are always located at the junction of the walls and the floor.
5. Law of orifices location 2: The orifices of the root canals are always located at the angles in the floor- wall junction.
6. Law of orifices location 3: The orifices of the root canals are located at the terminus of the root development fusion lines.
The LN bur (Caulk/ Denstply, Tulsa, OK, USA), the Mueller bur (Brasseler, Savannah, GA, USA) and thin ultrasonic tips are especially useful for locating calcified canals. Another important instrument for orifice location is the DG-16 explorer. At this point a fine instrument, usually a No. 8 or No. 10 K –file is placed into the orifice, and an attempt is made to negotiate the canal. An alternative option is to use instruments with reduced flute, such as a Canal Pathfinder (JS Dental, Ridgefield. Conn.) or instruments with greater shaft strength such as the Pathfinder CS ( Kerr Manufacturing Co.), which are more likely to penetrate even highly calcified canals.Remove the cervical ledge or bulge. If the orifice still cannot be negotiated with a fine instrument, drill 1-2 mm into the center of the orifice with a No.2 round bur on slow speed and use the explorer to re-establish the canal orifice. When counter- sinking or troughing in an area where an orifice is located, be sure the pulp chamber is dry. The bur rotating at a slow speed will remove whitish chips that then accumulate in the orifice. After a light stream of air is blown into the chamber, these chips appear as white spots on the dark floor of the chamber and serve as markers for exploration or further countersinking. This approach can be used if the fourth canal of the maxillary molar or a separation of the mesio-buccal and mesiolingual canals is anticipated in mandibular second molars.Recently a combination of access refinement ultrasonic tips and magnification has revolutionized the basic concept of access cavity preparation. The uncovering of the floor of the pulp chamber can be accomplished with the help of the CPR 2D or BUC 1 tips. The pulp stones sometimes can be vibrated or teased out by the CPR 2D or BUC 1 tips; at other times, they can be planed with the help of a BUC 2 tip- a process similar to planning the root surface. Grind the floor until the dark- colored dentine becomes visible. is of critical importance because it dictates and guides the extension of access cavity.13 Locating canals and initial penetration under the microscope is also aided by fine instruments like the Micro- Orifice Opener( Denstply Maillefer, Ballaigues, Switzerland.).
BIOMECHANICAL PREPARATION
Coronal flaring in a crown- down fashion is preferred.Incremental instrumentation is achieved by creating new increments between the established widths by cutting off a portion of the file tip, thus making it slightly wider in diameter. For example, if a 1 mm segment is clipped from a size 10 file, the instrument becomes a size 12, by trimming sizes 15, 20 and 25, instruments of sizes 17, 22 and 27 respectively can be created. In extremely sclerotic canals, only 0.5 mm segments are trimmed, increasing the instrument width by 0.01mm and making a size 10 into a size 11, etc. because cutting the shaft imparts a flat tip, a metal nail file is used to smooth the end and reestablish a bevel after the removal of any segment.6
CHELATING AGENTS-IS THERE ANY ROLE
Chelator preparations have been advocated frequently as adjuncts for root canal preparation, especially in narrow and calcified root canals. Apical dentin is more frequently sclerosed, and is more mineralized. The authors recommend liquid EDTA solution be introduced into the pulp chamber (pipette, cotton pellet ) to identify the entrance to calcified canals.14
TIME TO STOP LOOKING FOR CANAL
In the treatment of calcified canals it is common to find a total occlusion of the canal space at any level.11 Smith reviewed the literature concerned with calcific metamorphosis and collected the following data:
Calcified teeth that were not treated endodontically developed radiographic or clinical symptoms in upto 16% of the cases.
Studies of the success and failure of conventional endodontic therapy reported failure rates of 10% to 19%.
When these failure rates are compared, it appears that a calcified tooth treated endodontically would have no better chance of success than if it were left alone.8
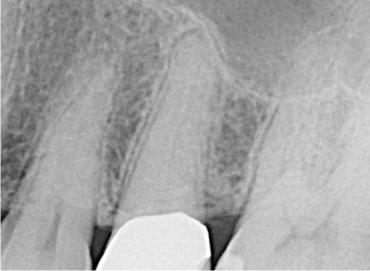 | Fig 1 :PRE-OPERATIVE
 |
 | Fig 2: POST-OPERATIVE
|
The patient reported with pain and swelling in 25
Fig 1 shows a case with calcified canal.
After locating the canal, final obturation was done. (Fig 2)
BIBLIOGRAPHY
1. Selden S. The role of dental operating microscope in improved nonsurgical treatment of “calcified” canals. Oral Surg Oral Med Oral Pathol 68:93-8, 1989.
2. Seltzer S, Bender.I.B. The Dental Pulp . Third edition 2000. MDMI inc.
3. Schafer.Textbook of oral pathology.
4 . Moss- Salentijn L, Hendricks- Klyvert M. Calcified structures in human dental pulps. Journal of Endodontics 14(4):184-189, 1988.
5. Neville .Oral and Maxillofacial Pathology. Second edition 2002. Saunders.
6. Weine F. Endodontic Therapy. Fifth edition.1996. Mosby.
7. Gutmann J.L, Dumsha T.C, Lovdahl P.E, Hovland E.J. Problem Solving in Endodontics: prevention, identification and management. Third edition. 1997 Mosby.
8. Amir F, Gutmann JL, Witherspoon D.E. Calcific metamorphosis: A challenge in endodontic treatment and diagnosis. Quintessence International 32:447-455, 2001.
9. Dodds N, Holcomb J. Endodontic management of teeth with calcific metamorphosis. The compendium of continuing education, 6 (7):515-51, 1985.
10. Selden S. The role of dental operating microscope in improved nonsurgical treatment of “calcified” canals. Oral Surg Oral Med Oral Pathol 68:93-8, 1989
11. Gutmann J.L, Dumsha T.C, Lovdahl P.E, Hovland E.J. Problem Solving in Endodontics: prevention, identification and management. Third edition. 1997 Mosby
12. Khabbaz MG, Serefoglou MH. The application of buccal object rule for the determination of calcified root canals.International Endodontic Journal 29:284-287, 1996.
13. Iqbal M K. Nonsurgical ultrasonic endodontic instruments. Dent Clin N Am 48 :19- 34. 2004.
14. Hulsmann M, Heckendorff M, Lennon A. Chelating agents in root canal treatment: mode of action and indications for their use. International Endodontic Journal, 36, 10- 830,2 003
|