Bad breath as they say is better than no breath at all. And as "George Orwell" said, "the road to wigan pier". You can have affection for a murderer, but you cannot have affection for a man/woman whose breath stinks.
Yet, halitosis is a common and universal problem that can lead to a significant amount of social disharmony and embarrassment1. Halitosis term originates from the Latin "halitus" means "breath" and the Greek "osis" means "abnormal" or "diseased".
In simple words also known as "Bad Breath, Foul Odor, Fetor ex ore, Fetor oris”
Introduction
Halitosis, breath malodor or colloquially known as "bad breath" can be subdivided as real halitosis, pseudohalitosis and halitophobia2.
True halitosis3
Real halitosis can be further subdivided into physiological and pathological halitosis. Physiologic halitosis includes halitosis caused by dietary components, deleterious habits, morning breath, secondary to xerostomia caused by physiologic factors. Pathologic halitosis occurs secondary to pathologic conditions or oral tissues like gingival and periodontal diseases like periodontitis, acute necrotizing ulcerative gingivitis, residual post-operative blood, debris under dental appliances, ulcerative lesions of the oral cavity, Halitosis may be associated with coated tongue, may occur due to xerostomia secondary to salivary gland diseases, tonsilloliths.
Pseudohalitosis3
Patients who suffer from pseudohalitosis complain of the existence of halitosis though it is not perceived by others. This condition can be managed effectively by counseling (using literature support, education and explanation of examination results) and simple oral hygiene measures.
Halitophobia3
Some individuals continue to insist that they have halitosis even after they have been treated for genuine or pseudo-halitosis. Such individuals are categorized as halitophobic. Halitophobia may be considered when no physical or social evidence exists to suggest that halitosis is present.
Psychogenic Halitosis3,4
Psychogenic Halitosis is the one which is imagined. In this a person believes that his breath smells bad when it actually does not. This problem may occur in people who tend to exaggerate normal body sensations. Sometimes this is caused by a serious mental disorder such as schizophrenia. A person with obsessional thoughts may have an overwhelmed sense of feeling dirty. A person who is paranoid may have the delusion that his organs are rotting. Both these persons feel their breath smells bad. Such people may be helped by having a doctor or dentist assures them that they do not have bad breath. If the problem continues, person benefit from seeing a psychotherapist.
The term oral malodor characterizes malodor that has its origin in the oral cavity. Clinical surveys have shown that over 90% of all breath malodor originates in the mouth5 (Delanghe et al 1997, van Steenberghe 1997).
History
The references of oral malodour have been found in scripts of Eber papyrus as early as 1550 B.C., and in the Talmud (a book containing ancient Jewish civil and religious law). Hippocrates (460-400 B.C.) had developed a mouthwash of unadulterated wine, anise, dill seed and myrtle. Maccius Platus (254-184 B.C.) a Roman dramatist who was sufficiently offended by his wife's halitosis to find it just cause for infidelity.5 In 19th century Joseph Howe, a physician, introduced his well-written and informative book. He believed that halitosis was the result of sulphuretted hydrogen, which is found in great abundance in the intestinal canal as well as in decayed teeth, dead teeth and inflamed gums. He also postulated that stress, in the form of fear, excitement or tension may sufficiently alter the body systems to produce a disagreeable breath odor.6
Epidemiology
Information regarding the prevalence of oral halitosis is scarce due to lack of epidemiological studies. An early study from The Netherlands among 11625 individuals revealed a prevalence of approximately 25% in subjects older than 60 years of age (de Witt 1966). In subjects under 20 years, the prevalence of oral halitosis was 10%, indicating that the prevalence of this condition increases with age. Several studies in industrialized countries report an incidence as high as 50%, with a various degree of intensity. In China the incidence of oral halitosis was surveyed in a sample of 2000 individuals aged 15-64 years. Oral halitosis was measured in 27.5%of the subjects with organoleptic measurements (Liu et al 2006).7 Bornstein et al. 2009 reported 20% prevalence of detected chronic halitosis among 626 male army recruits of Switzerland. Yokoyama et al (2010) reported 42% prevalence of halitosis experience (anxiety or consciousness of the problem at least once) and 39.6% prevalence of clinically detectable malodour in 474 senior high school students of Japan.8
Fact file
Breath smells only when certain aromatic compounds are found dissolved in it. These include methyl mercaptan, hydrogen sulphide, cadaverine, putrescine, skatole and isovaleric acid9.
Some of these may be absorbed from the bowel in the bloodstream and then circulated around the body until they are excreted via the lungs in the breath. In the same way garlic rubbed into the soles of feet can later be detected in trace amounts in the breath. Spicy foods also create recognizable odor in some people's pungent exhalations.
Etiology
Temporary halitosis: It results from hot/spicy food, certain drinks, alcoholic beverages, coffee and most common from garlic, onion, salty foods, spices, curries, cured foods like salamis and cooked food such as kippers10. Tobacco consumption causes mouldy odor and Hyposalivation/ Xerostomia (dry mouth) also leads to bad breath11.
Morning breath: Everybody has a degree of halitosis, first thing in the morning. There is a physiological reason for this. During sleep, the flow of saliva is reduced drastically and tongue and cheek move very little. This allows food residues to stagnate in the mouth and dead cells that are normally shed from the surface of tongue and gums and from the inside of cheek to accumulate. As bacteria starts to work on them and digest them, an unpleasant smell is generated. This process is biologically known as putrefaction/rotting.
Although normal, anyone suffering from nasal congestion whose mouth breathes is more likely to suffer from these actions to a greater extent. Luckily, this morning breath generally disappears after breakfast and after brushing the teeth because saliva starts to flow again and any left over residues are washed away and swallowed12.
Smoking (cigarettes/cigars): Breath smells like ash tray. Smoking also reduces the flow of saliva and therefore further exacerbates the problem13.
Crash dieting/fasting: When the body is no longer supplied with energy giving carbohydrates it first breaks down glucose stored in the muscles and liver in the form of glycogen. But this does not last long. After a few hours, the body begins to breakdown its fat stores and the waste product of their metabolism, ketones, endows the breath with a distinctive sweet and sickly smell. This can be seen in those who has vigorously worked out and exercised and not taken sufficient carbohydrates before or after. People on a strict caveman or high protein diet experience the same effect for similar reasons.
Oral Malodor
Bad breath is usually caused by bacteria that live in person's mouth. Bacteria, just like humans, go through their lives consuming food and excreting waste. The waste products produced by some oral bacteria are sulfur compounds. These odoriferous waste products usually lie at the root of person's bad breath problem.
The stench associated with rotten eggs is caused by hydrogen sulfide. The stinky smell emanating from feed lots and barnyards is one produced by methyl mercaptan and odor associated with ocean is that of dimethyl sulfide. Each of this is excreted as a waste product by bacteria that live in our mouths. Together dentist refer to them as Volatile Sulfur Compounds (VSC'S). Term volatile simply describes the fact that these compounds evaporate readily even at normal temperatures. The extreme volatility of these compounds explains how they have the ability to offend around us instantly.
Production of VSC's
The unpleasant smell of breath mainly originates from VSC's which comprise of hydrogen sulfide (H2S), methyl mercaptan (CH3SH), dimethyl sulfide (CH3)2SH, dimethyl disulfide (CH3)2S2, as first discovered by Tonzetich. They all are thiols; containing a characteristic -SH group which is formed when the oxygen atom in hydroxyl group is replaced by sulfur. Oral thiols are toxic byproducts of gram negative anaerobic bacterial metabolism of sulfur containing amino acids (cystine, cysteine and methionine) that reside in saliva, GCF, the gingival and periodontal pocket and tongue surface. This bacterial metabolism is of putrefactive nature and leads to oxygen depletion14.
Volatile fatty acids such as valerate, butyrate and propionate are all malodorous. When hormonal, gastro-intestinal, renal, or metabolic pathologies are the cause, additional malodorous molecules can be produced; these circulate in the blood and are expressed through the expired air or GCF.
Other waste products are
Cadaverine: Smell associated with corpses
Putrescine: Produced by decaying meat;
Skatole: Human faecal matter;
Isovaleric acid: Sweaty feet.
The above wonderful mixture of compounds emanates from mouth of human and no one is exception. Everyone has some level of these unpleasant compounds in their breath. Fortunately however, low levels of these compounds cannot be detected by human nose. It is only when the levels become elevated, others nose can detect them.
Bad breath is caused by waste products of anaerobic oral bacteria (more specifically gram negative anaerobic bacteria15 e.g.: prevotella intermedia, porphyromonas gingivalis etc.). Term anaerobic describes that they best grow in environments devoid of oxygen. Person's mouth is a home for hundreds of different species of bacteria and on going in our mouth is a constant battle for living space between type of bacteria which do create waste products that causes bad breath and those that don't and it's the precise balance between the relative number of these type of bacteria that determine the quality of person's breath.
Plaque accumulation (the whitish film that is formed above and below gum line and also on tongue) can tip the scales in favor of odor causing bacteria. A layer of plaque as thin as 0.1-0.2 mm becomes depleted to oxygen, precisely in which anaerobic bacteria flourish. So, as more and more plaque builds up, bacteria causing bad breath gain available living space and proliferate, thus increasing the level of odor. Solis-Gaffar et al. examined eight prominent Gram-positive and four Gram-negative bacteria for their ability to produce volatile sulfur compounds. All of the Gram-negatives and none of the Gram-positives produced H2S, CH3SH, and (CH3)2S6. Tonzetich and McBride examined strains of B. melaninogenicus for their ability to produce volatile sulfur metabolites and found collagenase and protease positive strains (asaccharolyticus) produced more of these cell and tissue destructive compounds than strains (var. melaninogenicus) that did not have collagenase and protease activities. F. nucleatum, an anaerobic Gram-negative rod, is another prominent organism in the microflora of the crevices of humans especially those with gingivitis/periodontitis that can metabolize cysteine and methionine and produce the sulfur volatiles that contribute to malodor.9
What is the food source for anaerobic bacteria that cause bad breath?
Most of the odoriferous compounds that cause bad breath are waste products created by anaerobic bacteria, as they digest proteins. This means that as we consume food items such as meat and fish, bacteria living in our mouth also get meal and waste products from their meals are precisely the compounds that cause bad breath. There is always naturally occurring protein food sources floating around in our mouth such as dead skin cells or protein compounds found in the saliva. And then also especially for those who are not diligent with brushing and flossing, there is always the left over food debris from yesterdays meal and the meal before that…..and the one before that…….
High protein foods include meat, fish, sea food and eggs; dairy foods such as milk, cheese, yoghurt; cereal grains and products; desserts especially cakes and pies.
Where do the bacteria that cause bad breath live?
For most of us bad breath causing bacteria live on the surface of tongue. Secondary locations can be at or below person's gum line16.
Bacteria that live on person's tongue
Most common odor producing region of the tongue is its posterior region. covered by a whitish layer, dental plaque and its chocked full of anaerobic bacteria that cause bad breath. The precise surface texture found on individual's tongue will influence the amount of coating that tends to accumulate. Fissured tongue, grooved tongue, and lingua plicata have more potential to accumulate bacteria laden coating than those with smoother tongue surface.
Refer table 1 for classification of severity and extent of tongue coating (Van Steenberghe, 2004). There is a direct correlation between the amount of coating that exists on persons tongue and total number of anaerobic bacteria17.
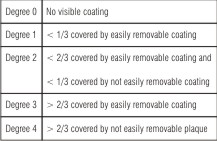 | Table 1 - Classification of severity and extent of tongue coating (van Steenberghe, 2004)
 |
Bacteria that live at and below person's gum line
When we floss the teeth, at times we are dredged up with foul taste or odor. This odor is more noticeable in the posterior part of the mouth, as the bacteria that cause bad breath often find a cozy home here.
Even in a relatively healthy mouth, anaerobic environment both around and in between the teeth and underneath the gum line can be found. This anaerobic environment is more in people who suffer from gum diseases such as gingivitis and periodontitis (Periodontal Disease). In periodontal disease the deep recesses of the periodontal pockets are difficult to clean. This creates the ideal anaerobic environment for the bacteria that causes bad breath.
Other reasons for oral malodor are Candidiasis, deep carious lesions (particularly after food impaction), exposed pulps and open root canals, extraction wounds, interdental food impaction, necrotizing ulcerative gingivitis (NUG), necrotizing ulcerative periodontitis (NUP), acrylic prosthesis and Vincent's angina.
Yoneda M et al have reported a case of oral malodor associated with internal resorption.18
Association of oral malodor with periodontitis
A correlation has been found between VSC concentration in mouth air and increased pocket depth in periodontitis patients.19,20 The uptake of volatile sulphurs by epithelial cells may play an important role in the pathogenesis of periodontal disease: it has been proposed that volatile sulphurs may alter the permeability of affected cells and facilitate the access of toxic metabolites into the underlying connective tissue thereby contributing to collagen degradation. There is also general agreement that the VSC content of exhaled mouth air and the concentration of VSC precursors increases with the severity of periodontal disease.21
Source of VSC production in periodontitis patients12
In 1998, Yaegaki et al carried out a study aimed to investigate the VSC production of tongue coating in relation to the severity of periodontal disease. They analyzed the VSCs in mouth air using gas chromatography before and after removing the tongue coating. They concluded the tongue coating might be a main site of oral malodor production in slight or moderate periodontal disease, whereas, the periodontal pocket would be the main origin of VSCs only in severe periodontal disease.
Role of VSCs in the pathogenesis of destructive periodontitis
In addition to being a major contributor to oral malodor, VSCs have been implicated in the disruption of oral mucosa and may contribute to the progression of periodontal disease. Some studies suggest that the production of VSCs by these microorganisms may contribute to the progression of periodontal disease via breakdown of the oral mucosa leading to bacterial invasion. Ng and Tonzetich found that the permeability of porcine sublingual mucosa increased 75 percent and 103 percent following exposure to hydrogen sulfide and methyl mercaptan, respectively. This finding suggests that the VSCs of oral malodor could contribute to the pathogenesis periodontitis.22
VSCs are highly toxic to tissues even at extremely low concentrations and, therefore, may play a role in the pathogenesis of inflammatory conditions affecting the periodontium, such as periodontitis. They also alter the metabolism of fibronectin and interfere in the enzymatic and immunological reactions leading to tissue destruction while showing an increase in the release of Interleukin-1 (IL-1) and PGE2 .12
Some studies have failed to demonstrate positive correlations between periodontitis severity and halitosis. Rosenberg M et al (1991)23 found a weak correlation between presence of pockets greater than 7 mm and sulphide measurements. Bosy et al in 1994 did not find a relationship between periodontal disease and the prevalence or severity of halitosis. In addition to the lack of presence/absence of periodontal disease, the intensity of halitosis based on VSC concentration was 19% less in periodontally healthy subjects (mean 111 ppb) than in subjects with periodontitis (mean=136 ppb).21
Malodor of Extraoral Origin3,4,24
In only 10% of cases, cause can be traced back to an internal (Lang and Filippi, 2005a) or ENT problem (Tonzetich, 1978)
Refer table 2 for the possible causes. Certain breath odors are of diagnostic significance for the physician. For example, the acetone odor of diabetic ketoacidosis, the ammonia smell of uremia and the rotten egg smell of liver failure is due to the inability of the liver to break down diethyl sulfide, which is released due to bacterial action. This is excreted through the lungs.
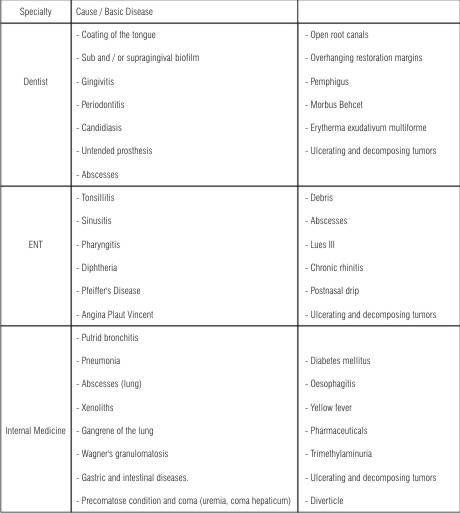 | Table 2 – Possible causes of Halitosis
|
Halitosis of Upper Respiratory Tract: It may be because of chronic sinusitis, nasal obstruction, nasopharyngeal abscess and carcinoma of the larynx.
Halitosis of Lower Respiratory Tract: It may be because of bronchitis, bronchiectasis, pneumonia, pulmonary abscess and carcinoma of the lungs (Attia and Marshall1982, Lu 1982, Durham et al 1993, McDowell and Kassebaum 1993)
Gastrointestinal tract:
Unpleasant odor from the lower gastrointestinal tract is only detectable during belching or vomiting, because the esophagus is normally collapsed (Attia and Marshall 1982). The stomach is therefore not considered to be contributory to the halitosis, except in rare circumstances (Rosenberg 1996). The following pathologies might be responsible for less than 1% of malodor cases:
Zenker's Diverticlum:
It is hernia in esophageal wall, allowing accumulation of food and debris and thus putrefaction. It can cause a significant breath odor because it is not separated from oral cavity by any sphincter.
Gastric hernia:
Fundus of stomach protrudes through diaphragm with relative sphincter insufficiency allowing gases to escape and contents to flow back to the esophagus can cause reflex of the gastric contents up to the oropharynx. This is sometimes combined with ructus, where air from stomach suddenly regurgitates.
Gastric Reflux:
It is a common cause of morning halitosis. In this, there is reflux of gastric juice, bacteria and digested food into the pharynx.
Intestinal gas production:
Others:
Extraoral halitosis might also be a manifestation of a serious systemic disease, such as hiatus hernia, hepatic cirrhosis or diabetes mellitus (Tangermann 2002). Tangerman A, Winkel EG (2007) provided evidence that the VSC, CH3SH and to a lesser extent H2S are the main contributors to intra-oral halitosis and that CH3SCH3 is the main contributor to extra-oral or blood-borne halitosis, due to a hitherto unknown metabolic disorder.25
Rosenberg M et al (2007)26 identified predictive factors for bad breath in the general adult population, by a 38-question self administered questionnaire, along with objective odor judge and instrumental measurements and results suggested that that alcohol intake and body mass index may be factors that help predict oral malodor.
Medications:
Some drugs, such as metronidazole, can cause breath malodor. Metronidazole, an antimicrobial, also leads to the patient's perception of metallic taste, which is often confused with breath odor. Eucalyptus containing medications impart a melon like odor. Arsenic smells of rotten onions. Amitriptyline (a tricyclic anti-depressant), certain anti-hypertensives, sedatives, hypnotics, anti-allergic drugs which dry up saliva as a side effect, also add to the problem.
Do You Have Bad Breath?
At some point each of us had bad breath. For any individual, the exact status of their breath is difficult to ascertain, reason for this is that the oral cavity, the source of our breath, is connected to our nose by way of an opening which lies in the back of our mouth (back in the region of soft palate). Since noses tend to filter out and ignore background odors, it filters out and ignores our own bad breath. This means it is quite possible for a person to have bad breath, yet not be aware of it.
Diagnosis
Patient's History
-
Patient should be asked to describe the type of smell that is being noticed. Depending on the origin, different smells may be distinguished. (Refer table 3)
-
Who noticed the bad breath- patient himself (halitophobia / pseudohalitosis) or others?
-
Under which circumstances was the bad breath experienced? Only in the morning (temporary bad breath), after meals (due to certain foods or spices), or after lying down. Halitosis after meals or lying down may be indicative of regurgitation oesophagitis (Van Steenberghe, 2004).
-
The clinician should ask about the frequency (e.g., every month), time of appearance with in the day (e.g., after meals can indicate a stomach hernia) etc. One of the major challenges in judging halitosis is that self reported halitosis is quite subjective. Thus, it may be helpful if the patient is accompanied by candidate who is able to give more objective picture. For example, a spouse, friend or family members.
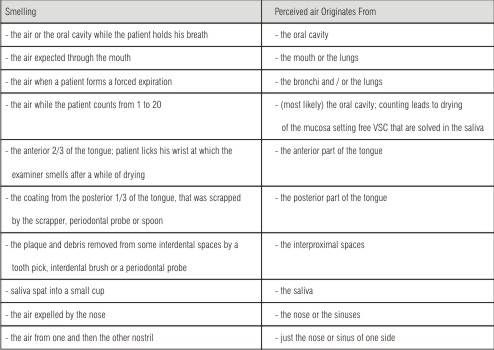
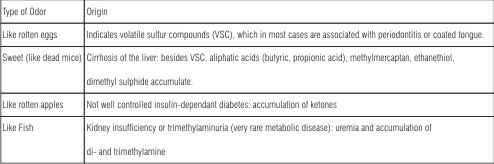 | Table 3 - Different types of breath malodor according to their most likely origin (Preti et al, 1992; van Steenberghe, 2004)
|
Is there a way a person can test their own breath24?
There are indirect routes to test your own breath.
Experiment 1:Lick your wrist, wait about five seconds while the saliva dries somewhat and then smell it. This experiment tells us about the smell of the anterior portion of the tongue.
Experiment 2:Take a spoon. Turn it upside down and use it to scrap the very back portion of the tongue. Take the look at the material that has been scraped off, usually a thick whitish material. Now take a whiff of it. This experiment tells us about the smell of posterior portion of the tongue. This smell is probably the way your breath smells to others.
Experiment 3:Take a toothpick and introduce into the interdental area (area between teeth) and smell it.
Experiment 4:Spit saliva in a small cup or spoon. Allow it to dry for a few seconds (so that putrefaction odors can escape from the liquid) and then smell it.
How Academic Researchers Test for Bad Breath?
Before a dental researcher can evaluate various cures for bad breath, they must measure its severity both initially and after the cure.
Organoleptic Testing4,24
Gold standard for measuring halitosis is organoleptic testing. In this testing, the researchers are using their senses of smell i.e. their nose as the means for making the determination. Historically, this method has been a frequent choice among dental researchers. Noses are readily available, inexpensive to obtain and operate and to their credit, noses can detect up to 10,000 different smells. One of the problems associated with using this method is that it is not totally objective. Another is that factors other than just breath odors can and do influence organoleptic evaluations. Factors such as hunger, menstrual cycle, head position and the degree of attentiveness and expectation can each influence a judge's interpretation of what they smell.
To assess halitosis, examiner should be trained and calibrated. To assess examiners differentiation abilities, test kits with different scents may be used (smell identification test). Further, these kits containing different dilutions of specific scents are available to assess and train differentiation strength of scents (Lang and Filippi, 2005b). Sometimes, the examiner's smell may be impaired due to ones own halitosis, or temporary deterioration of smelling (example rhinitis).
Prerequisites: Going to the dentist to classify the halitosis can be quite embarrassing, so high level of privacy has to be maintained. Patient and examiner have to abstain from substances that cause temporary malodor, 12 hours before the examination. Substances that mask halitosis may have to be avoided (e.g. shampoo, perfume, mouth rinses). Classify it in four degrees of severity (Refer table 4). Further the clinical examination should follow a certain sequence in order to distinguish the origin of malodor (Table 5).
Demerits: Each judge participating won't be able to make equivalent comparison. And when we are repeatedly exposed to a bad odor our sense of smell acclimates to the odor and therefore loses much of its sensitivity. Bad breath that was exceedingly objectionable at the beginning, may seem quite less as the evaluation continues.
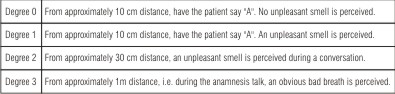 | Table 4 - Classification of Subjectivity perceived Halitosis (Seemann, 2002)
|
 | Table 5- Sequence of the clinical examination
|
Instrument assessment24
It has been used by dentist to study bad breath and definitely quantify the precise level of specific compound present in someone's breath. This device can analyze air, (incubated) saliva, or crevicular fluid for any component.
Use: Primarily for scientific purpose.
Demerits: Relatively expensive, requires personnel with special training to operate them, not portable equipment and time consuming.
Recently a small, portable gas chromatograph (Oral Chroma, Abilit, Henderson, Nevada) has been introduced, which makes this technique available for periodontal clinics. It has the capacity to measure the concentration of three key sulfides separately.
Halimeter4,24
It is a specialized type of sulfide monitor and it produces a mean by which tester can quantify degrees of bad breath in parts per billion (ppb). These machines first introduced in 1991, measure the level of sulfide gas found in persons breath i.e. VSC'S. Halimeters showing high levels of sulfide suggest a correlating high levels of VSC although doesn't test for individual type of VSC's specifically.
The examination should preferably be done after at least 4 hours of fasting and after keeping the mouth closed for 3 minutes. The mouth air is aspirated by inserting a drinking straw fixed on the flexible tube of the instrument. This straw is kept about 2cm behind the lips, without touching any surface and while the subject keeps the mouth slightly open and breathes normally.
Absence of breath malodor leads to readings of 100 ppb or lower. Patients with elevated levels of VSC's easily reach 300-400 ppb.
Disadvantages: It test for a fewer no. of compounds (sulfides only) than gas chromatographs and in fact tests for no individual compounds at all but just sulfide as a class. Additionally compounds such as ethanol (alcohol) and essential oils (both of which are found in mouthwashes) interfere with halimeters ability to make a measurement.
Advantages: It requires no special training to use, is portable, measurements can be made quickly and apparatus is comparatively inexpensive.
Uses: For follow ups, psychological support during treatment and many patients trust the result of a device more than dentists nose (Seeman 2002).
Rosenberg M et al (1991)23 elucidated that although assessment of steady-state sulphide levels by the sulphide monitor does not constitute a direct measure of oral malodor, its relation to organoleptic measurement, superior reproducibility, objectivity, and sensitivity support the use of the sulphide monitor in clinical studies. Based on the superior reproducibility and sensitivity of the sulphide measurements compared with organoleptic measurements, the sulphide monitor may be a valuable tool for assessment of oral malodor. The sulphide monitor also presents other advantages such as: (i) no need for skilled personnel; (ii) non-invasive; (iii) low likelihood of cross-infection; (iv) portability; (v) relatively inexpensive; and (vi) rapid turnaround time of one to two min between measurements. However, it lacks the specificity of gas chromatography, since it cannot distinguish between the proportions and species of different VSC's.
The BANA Test
Bacteria that produce bad breath can be detected by performing BANA test. Bacteria, in question have the characteristic of being able to produce an enzyme that degrades the compound BANA (benzoyl-D, L-arginine-napthylamide). When sample of patient's saliva that contains these bacteria is placed in the BANA testing compound, they cause it to break down. As a result, the testing compound changes color. The results of a study by Kozlovsky A et al (1994) suggested that the BANA test, a simple, adjunct assay together with volatile sulphide determination which provides additional quantitative data contributing to the overall association with odor judge estimation.27
Utilizing Chemiluminescence
One of the most recent methods for detecting the compounds associated with bad breath. Method was introduced in 1999. When a sample containing sulfur compound is mixed with the tests mercury compound, the resulting reaction causes fluorescence.
Advantage: It provides better selectivity and sensitivity when measuring low levels of sulfur compounds as compared to halimeters.
Zinc oxide and Nitrogen chemiluminescence detectors
These chemiluminescence detectors permit the precise measurement of nitrogen compounds such as indole & cadaverine in organic matrices. This helps to determine whether these nitrogen compounds are present in mouth air.28
Electronic Noses
Also called as Artificial Noses, are supposed to provide quantification and classification of exact smells (Shimura et al, 1997). Originally it was developed for quantitative assessment of smells in food or beverage. However, an application to diagnosis of halitosis appears reasonable.
Dark Field or Phase- Contrast Microscopy24
Gingivitis and periodontitis are typically associated with a higher incidence of motile organisms and spirochetes. These can be seen directly with the help of microscope.
Advantage: patients become aware of the bacteria present in the plaque, tongue coating and saliva.
How do you cure bad breath?
The most important step a person can take towards improving the quality of breath is to clean their mouth in a manner which helps to minimize the amount of food available for anaerobic bacteria, minimize the total number of these bacteria that exist, minimize the availability of type of environment in which these bacteria prefer to live, make any environment in which these bacteria do live less hospitable. On a second front, a person can use products that neutralize the odor causing volatile sulfur compounds.
Minimizing the food supply for bacteria that causes bad breath
When anaerobic bacteria digest proteins, volatile sulfur compounds are created as waste products that cause bad breath. The person who maintains a vegetarian diet mostly of fruits and vegetable has fewer chronic breath problems than those who consume protein rich food such as meat.It is important for a person to clean one's mouth thoroughly especially after eating protein rich food. This is because even after we have finished a meal minute particles of food still remain in our mouth. Much of this food debris ends up lodged between our teeth and incorporated into the coating found on the posterior part of our tongue. Since these are precisely the same locations in which the anaerobic bacteria that cause bad breath live, if a person does not clean their mouth thoroughly a food supply is provided for these bacteria over an extended period of time.
How cleaning your teeth and gums can help to cure bad breath?
As already explained the bacteria that causes bad breath live in dental plaque that accumulates on and around person's teeth, both at or below gum line. So a thorough brushing and flossing technique is needed in order to remove this plaque and any food debris.
Make an appointment with your dentist
If bad breath problem persists, even after a period of following all of the tips and suggestions, then one should schedule an examination and cleaning appointment with the dentist so that one can discuss their problems with them. During this visit the following can be accomplished:
1.) Sometimes effective brushing and flossing technique can be difficult to learn. After examining, dentist can provide with instructions, tips, and pointers that will be helpful in specific situation.
2.) Tartar (dental calculus) accumulation can interfere with effective brushing and flossing. Scaling and root planing will remove this debris from teeth. In a study by Saito Mitsuhiro et al (2000) halitosis parameters as measured by the Halimeter, and the organoleptic examination were improved, and the total amount of plaque was decreased. These results suggest that improved gingival inflammation with periodontal treatment improves halitosis.29
3.) Periodontal evaluation: Periodontal pockets are often impossible for us to clean for bacteria to live. So, if periodontal condition is evaluated, dentist can outline the treatment required to control this condition.
4.) Dentist will check if there are any untreated dental conditions that could be causing or exaggerating breath problems.
5.) Dentist will help you to determine whether its oral or medical evaluation is indicated.
Bad Breath Cures by Tongue Scrapers or Tongue Brushes1
Most people overlook cleaning their tongue, however, starting to do so on a regular basis, can be the single most beneficial treatment for bad breath that a person can institute. The anterior portion of a person's tongue is usually less offensive than the smell found emanating from the posterior part. The reason for this is related to the fact that the anterior portion of the tongue is somewhat self-cleansing and more exposed to outside environment, thus getting a better oxygenation and therefore less likely to harbor large numbers of odor producing bacteria. Many tongue functions require that the anterior portion of the tongue touches firmly against the hard palate. This friction produces a cleansing action, therefore preventing any significant bacterial accumulation.
The posterior portion of the tongue in comparison only rubs up against the palate (soft palate) relatively gently during tongue movements. This soft palate contact does not provide enough friction to produce any significant cleansing. For this reason it is typically the posterior aspect of the tongue that is found to harbor the bacteria that cause a person's bad breath, and thus the posterior tongue is the most important area to clean.
By Tooth Brush:
To do so, start as far back as possible and then make brush strokes outward, toward the front of mouth. One needs to use some pressure but of course not enough to cause irritation to tongue. As a way of improving the effectiveness of tongue brushing efforts, one can use toothpaste.
By Tongue Scraper:
Some people believe this is more effective method and produces less gagging. To do so, place a tongue scraper on the posterior part of tongue. Be thorough and gentle and don't scrap so hard or vigorously that it irritates the tongue. Faveri M et al (2006) suggested that tongue scraping appears to be the most important hygienic procedure to reduce morning bad breath in periodontally healthy subjects.30
A Cochrane review (2008)31 conducted to provide reliable evidence regarding the effectiveness of tongue scraping versus other interventions (including mouthwashes) to control halitosis concluded that there is weak and unreliable evidence to show that there is a small but statistically significant difference in reduction of VSC levels when tongue scrapers or cleaners rather than toothbrushes are used to reduce halitosis in adults. They found no high level evidence comparing mechanical with other forms of tongue cleaning. Tongue scrapers or cleaners are slightly more effective than toothbrushes as a means of controlling halitosis in adults. This review, which included 2 trials (40 participants) found that, although the use of tongue scrapers was generally well accepted, the effects of tongue cleaning using scrapers or brushes appeared to be very short lived and there was some limited evidence of tongue trauma which occurred with prolonged use of one tongue scraper.
A study by Casemiro LA et al (2008)32 compared the effectiveness of a new manual toothbrush that has a tongue scraper on the back of its head and a commercial tongue scraper in improving breath odor and reducing the aerobic and anaerobic microbiota of tongue surface. They demonstrate that the adoption of methods for tongue cleaning associated to toothbrushing minimizes halitosis and reduces bacterial counts on tongue surface. The evaluated methods (toothbrush with a tongue scraper on the back of its head and conventional tongue scraper) were equally effective in the improving breath odor and reducing the facultative aerobic and anaerobic microbiota on tongue surface of the studied population.
Bad Breath Cure by Chemicals24
Mouthwashes, when used in conjunction with a regimen of effective tongue cleaning, tooth brushing, and flossing, can play a role in the treatment of bad breath. Carvalho MD et al (2004)33 demonstrated the beneficial impact of mouthrinses on morning breath even in the absence of mechanical plaque control. In a cross-over trial conducted by them on college students, the VSC formation was inhibited in descending order, 0.2% chlorhexidine, 0.12% chlorhexidine, triclosan and essential oils and cetylpyridinium chloride.The effectiveness of a particular mouthwash will be founded on its possessing one or both of the following characteristics:
A) Antibacterial mouthwashes
If a mouthwash has the ability to kill bacteria, so reduces anaerobic bacteria that produce VSC's and hence bad breath.
B) Mouthwash that neutralizes VSC's
The ingredients found in some mouthwashes have the capability to neutralize VSC's and/or the compounds from which they are formed.
Some of the different types of over-the-counter mouthwashes have been employed in the treatment of bad breath (Table 6). Following are the compounds which offer a great help to reduce the oral malodor:
1. Chlorhexidine: it is most effective anti- plaque and anti-gingivitis agent. Its antibacterial action can be explained by disruption of the bacterial cell membrane by the chlorhexidine molecules, increasing its permeability and resulting in cell lysis and death. Rosenberg et al showed that a 0.2% chlorhexidine rinse provides 43% reduction in VSC levels and a greater than 50% reduction in organoleptic mouth odor ratings.
2. Halita, a new solution containing 0.05% chlorhexidine, 0.05% CPC, 0.14% zinc lactate and no alcohol, has been found even more effective than chlorhexidine alone, suggesting that the other compounds are also important. This is explained by the synergistic action of chlorhexidine and CPC on one hand and by the zinc ions on the other hand.
3. Essential oils containing mouthwash present in market is Listerine. It has been found only relatively effective against oral malodor (25% reduction vs. 10% for placebo). In a study by Pitts G et al an essential oil mouthrinse was able to reduce the offensive gases present in morning bad breath as measured by a sulfide monitor, a result that is in agreement with those of a previous short-term study, in which the results indicated a reduction of the organoleptic scores by essential oils, which caused a sustained reduction in the plaque odorigenic bacteria, unlike the placebo.34 An argument was made that the re-odoration was important to the overall activity of the product only for about 30 min after treatment and, at post-treatment times of 60-180 min, the anti-odor activity of the product was due to its anti-microbial action. That conclusion became the basis for the premise that anti-VSC agents would succeed if they had an antimicrobial component.35
4. Chlorine Dioxide it is a powerful oxidizing agent that can eliminate bad breath by oxidation of hydrogen sulfide, methylmercaptan and the amino acids methionine and cysteine. Shinada K et al (2010)36 showed that a mouthwash containing ClO2 improved morning bad breath measured with the organoleptic measurement and reduced the concentrations of H2S, CH3SH and (CH3)2S measured by gas chromatography in healthy subjects. Moreover ClO2 mouthwash used over a 7-day period was effective in reducing plaque, tongue coating accumulation and the counts of Fusobacterium nucleatum in saliva.
5. Two- Phase Oil-Water Rinse Rosenberg et al designed a two-phase oil-water rinse containing CPC that was shown to result in daylong reduction in oral malodor. The efficacy of this formulation is thought to result from the adhesion of a high proportion of oral microorganisms to the oil droplets, which is further enhanced by the CPC. These reductions were almost comparable to chlorhexidine, superior to Listerine and significantly superior to a placebo.
6. Triclosan a broad spectrum antibacterial agent has been found to be effective against most oral bacteria and has a good compatibility with other compounds used for oral home care. The anti -VSC effect depends strongly on its solubilizing properties. In the Carvalho et al. (2004)33 investigation, plaque formation was not always directly associated with VSC measurements, since the triclosan and CPC mouthrinses were more effective in reducing bad breath than in reducing supragingival plaque accumulation. Therefore, it could be postulated that the superior reducing effect of these specific mouthrinses on bad breath may be related primarily to their efficacy in reducing the load of VSC-related microorganisms and oral debris in the whole mouth niches rather than only in supragingival plaque reduction.35
7. Amine fluoride / Stannous Fluoride
8. Hydrogen peroxide 3%
Quirynen M et al (2002)37 demonstrated that morning halitosis can be successfully reduced by the sole twice daily use of 0.2% chlorhexidine (CHX)-alcohol mouthrinse, 0.05% CHX +0.05% cetylpyridinium chloride (CPC) + 0.14% zinc lactate mouthrinse, an amine fluoride/stannous (AmF/SnF2) fluoride (125ppm F-/125ppm F-) containing mouthrinse, which all significantly reduced the bacterial load in the saliva and retarded the de novo plaque formation. The subjective ratings of the subjects were in general more in favour of CHX-CPC-Zn or AmF/SnF2 solutions.
Cochrane review investigating the effects of mouthrinses in controlling halitosis which included five trials (293 participants), found that there is some evidence that mouthrinses containing antibacterial agents such as chlorhexidine and cetylpyridinium chloride or those containing chlorine dioxide and zinc can to some extent reduce the unpleasant odour but the use of mouthrinses containing chlorhexidine resulted in noticeable but temporary staining of the tongue and teeth.38
Herbal remedies
Many natural products like yogurt, lemon water, mint leaves, vinegar, cardamom seeds are beneficial in curing bad breath.
Lodhia P et al (2008)39 have shown significant effectiveness of green tea in reducing oral malodor because of its disinfectant and deodorant activities, although effect was maintained for a very short duration. Green tea was found even more effective than sugarless chewing gum and mint in reducing volatile sulphur compounds.
Epigallocatechin gallate (EGCg), the main antimicrobial tea catechin, has been reported to inhibit growth and virulence factors of oral pathogens in vitro. Although the mechanism is unclear, the potential of EGCg in reducing halitosis caused by volatile sulfur compounds (VSCs) has been suggested. Xu X (2010)40 study tested the hypothesis that EGCg reduces VSCs by suppressing mgl, the gene encoding L-methionine-α-deamino-γ-mercaptomethanelyase, responsible for methyl mercaptan (CH3 SH) production by oral anaerobes. They concluded that EGCg may represent a natural and alternative agent to the antimicrobial chemicals.
Can breath mints, lozenges, drops, sprays, and chewing gum help to cure bad breath?
These products when used alone are not as effective as when used in conjunction with tongue cleanser, toothbrushes and flossing, especially when they contain agents that have the ability to neutralize VSC's. As an added benefit, the use of mints, lozenges and chewing gums will stimulate the flow of saliva in person's mouth and saliva has cleansing and diluting effect on the bacteria and bacterial waste products that are found in person's mouth and therefore, helps to minimize person's problems.
Role of dentifrices
Feng X et al (2010)41 conducted four randomized and controlled clinical trials and; meta-analysis evaluating the collective outcomes of four independent trials furnish evidence of significant short-term, overnight and cumulative breath malodor reduction after brushing with a stannous-containing sodium fluoride dentifrice that simultaneously provides additional cosmetic and therapeutic oral health benefits.
Peruzzo DC et al (2007)42 evaluate the effect of the flavoring agents present in a dentifrice on the formation of VSCs in the morning breath of healthy individuals and suggested that a flavor containing dentifrice seems to prevent VSCs formation in morning bad breath regardless of the amount of TC in periodontally healthy subjects.
How to clean dentures to reduce the menace?
Dentist should provide with specific instructions regarding the cleaning of dentures since dental plaque forms on dentures just like it does on teeth, gums and tongue. So, usually a dentist's recommendations will include instructions about thoroughly scrubbing your dentures with a toothbrush or specialized denture brush, both inside and out. After scrubbing, they might be placed in antiseptic solution.
For ENT and Medical Problems
For infections in nose, paranasal sinuses and pharynx: Appropriate antibiotic therapy.
For Gastric Reflux: Antacids, H2 blockers and appropriate changes in dietary habits.
A simple classification with corresponding treatment needs was reported by Miyazaki et al.2,35 Ken Yaegaki, Jeffrey M. Coil, (2000)2 suggested that treatment of physiologic halitosis (TN-1), oral pathologic halitosis (TN-1 and TN-2) and pseudo-halitosis (TN-1 and TN-4) would be the responsibility of dental practitioners. Oral pathologic halitosis is caused mainly by periodontal disease, a condition managed by periodontal treatment. Additionally, dental treatment may be necessary to correct faulty restorations that might contribute to poor oral health (TN-2). Furthermore, patients with genuine halitosis who undergo successful reduction of halitosis by TN-2 or TN-3 yet still believe that they have the condition should also be referred to a psychological specialist (TN-5).
Halitophobic patients usually refuse to visit a psychological specialist, because they cannot recognize their condition as psychosomatic. They never doubt that they have offensive oral malodour. Hence, they are unhappy with the dental clinician who tells them they do not have the condition. Some clinicians may hesitate to refer such patients to a specialist, and the patients may then start "doctor shopping." It is important, therefore, to provide TN-4 counselling to these patients.
Pseudohalitosis almost always requires referral for clinical psychologist management. In extreme instances, patients become socially isolated, may have their teeth extracted and occasionally commit suicide. However, patients often refuse to acknowledge that they may have a psychological problem. Therefore, the involvement of a third party (e.g. a confidant such as a close family member or a trusted friend) in the management may provide the patient with additional psychological support to consider the problem in a more objective manner2
General points to remember as Bad Breath Remedies
-
Drink plenty of water.
-
Rinse your mouth with water often.
-
Stimulate your mouth's flow of saliva.
-
Clean your mouth well especially after eating high protein content food.
Conclusion
Oral malodor (halitosis or bad breath) is an offensive odor of oral cavity and may disturb interpersonal communication and social activities. The oral region is the most frequent origin of halitosis. Factors associated with oral malodor were oral hygiene, periodontal disease and oral dryness. Hence health education and preventive intervention; such as tooth brushing instruction, and treatment regimens targeting periodontal disease as well as tongue cleaning should be incorporated to reduce levels of these compounds in mouth air and are satisfactory for cosmetic treatment.
References
1. Pedrazzi V, Sato S, Chiarello de Mattos MG, Guimaraes Lara EH, Panzeri H. Tongue cleaning methods: A Comparative Clinical Trial Employing a Toothbrush and a tongue scraper. J Periodontol 2004; 75:1009-1012.
2. Yaegaki K, Coil JM. Examination, classification and treatment of halitosis; clinical perspectives. J Can Dent Assoc. 2000; 66: 257-261.
3. Ongole R1, Shenoy N. Halitosis: Much beyond oral malodor. Kathmandu University Medical Journal 2010; 8:269-275
4. Scully C, Greenman J. Halitosis (breath odor). Periodontol 2000 2008;48:66-75
5. Rosenberg M, Septon I, Eli I, et al. Halitosis measurement by an industrial sulphide monitor. J Periodontol 1991; 62:487-489.
6. Bosy A. Oral Malodour: Philosophical and Practical Aspects. J Can Dent Assoc 1997;63(3):196-201
7. Edwin G. Winkel. Halitosis control: In Clinical Periodontology and Implant Dentistry by Jan Lindhe. 2008; Vol 5.1325-1340.
8. Rosing CK, Loesche W. Halitosis: an overview of epidemiology, etiology and clinical management. Braz Oral Res. 2011 Sep-Oct;25(5):466-71
9. Kleinberg I, Westbay G. Oral Malodor. Crit Rev Oral Biol Med 1990; 1:247-259.
10. Scully C, el-Maaytah M, Porter SR, Greenman J. Breath odor: etiopathogenesis, assessment and management. Eur J Oral Sci. 1997; 105: 287-293.
11. Koshimune S, Awano S, Gohara K, Kurihara E, Ansai T, Takehara T. Low salivary flow and volatile sulfur compounds in mouth air. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:38-41.
12. Sanz M, Roldán S, Herrera D. Fundamentals of breath malodour. J Contemp Dent Pract. 2001; 15:1-17.
13. Morita M, Wang HL. Relationship of sulcular sulfide level to severity of periodontal disease and BANA test. J Periodontol. 2001; 72: 74-78.
14. Silvia Rolda´n, David Herrera, Isabel Santa-Cruz1, Ana O'Connor. Comparative effects of different chlorhexidine mouth-rinse formulations on volatile sulphur compounds and salivary bacterial counts. J Clin Periodontol 2004; 31: 1128-1134.
15. Hawxhurst DC. Offensive breath: Dent Register 1873;27:104-110
16. Rosenberg M. Clinical assessment of bad breath: Current concepts. J Am Dent Assoc 1996; 127:475-482.
17. Perry A. Ratcliff and Paul W. Johnson. The Relationship between oral malodor, gingivitis and periodontitis. A review. J Periodontol 1999; 70:485-489.
18. Yoneda M, Naito T, Suzuki N, Yoshikane T, Hirofuji T. Oral malodor associated with internal resorption. J Oral Sci 2006;48 (2):89-92
19. Ratcliff PA, Johnson PW. The relationship between oral malodor, gingivitis and periodontitis: a review. J Periodontol 1999;70:485-489
20. Morita M, Wang H-L: Association between oral malodor and adult periodontitis:a review. J Clin Periodontol 2001; 28: 813-819.
21. Bosy A, Kzilkami GV, Rosenberg M, McCulloch CAG. Relationship of oral malodor to periodontitis: evidence of independence in discrete sub-populations. J Periodontol1994; 65: 37-46.
22. Klokkevold PR. Oral malodor: a periodontal perspective. J Calif Dent Assoc. 1997 Feb; 25(2):153-9.
23. Rosenberg M, Kulkarni GV, Bosy A, McCulloch CAG. Reproducibility and sensitivity of oral malodor measurements with a portable sulphide monitor. J Dent Res 1991; 70(11):1436-1440
24. Quirynen M, Van Steenberghe D. Oral Malodor: In Carranza's Clinical Periodontology 2006; vol 10. p 330-342
25. Tangerman A, Winkel EG. Intra- and extra-oral halitosis: finding of a new form of extra-oral blood-borne halitosis caused by dimethyl sulphide. J Clin Periodontol 2007; 34: 748-755.
26. Rosenberg M, Knaan T, Cohen D. Association among Bad Breath, Body Mass Index, and Alcohol Intake. J Dent Res 2007 86: 997-1000
27. Kozlovsky A, Gordon D, Gelernter I, Loesche WJ, Rosenberg M Correlation between BANA test and oral malodor parameters. J Dent Res 1994; 73(5): 1036-1042
28. Moss S. Halitosis and oral malodour. FDI World 1998; 5: 14-20.
29. Mitsuhiro S, Misaki O, Shuichi S, Yuko H, Keiko M, Reiko H, Akira H. A Study of the Treatment of Halitosis by Plaque Control. Odontology 2000;87(4):582-586
30. Faveri M, Hayacibara MF, Pupio GC, Cury JA, Tsuzuki CO, Hayacibara RM. A crossover study on the effect of various therapeutic approaches to morning breath odour. J Clin Periodontol 2006; 33: 555-560.
31. Outhouse TL, Al-Alawi R, Fedorowicz Z, Keenan JV. Tongue scraping for treating halitosis (Review); Cochrane Database Syst Rev. 2008; 8(4):CD005519.
32. Casemiro LA, Martins CHG, Carvalho TC de, Panzeri H, Lavrador MAS, Pires-De-Souza F de CP. Effectiveness of a new toothbrush design versus a conventional tongue scraper in improving breath odor and reducing tongue microbiota. J Appl Oral Sci. 2008;16(4):271-4
33. Carvalho MD, Tabchoury CM, Cury JA, Toledo S, Nogueira-Filho GR: Impact of mouthrinses on morning bad breath in healthy subjects. J Clin Peridontol 2004; 31:85-90.
34. Pitts G, Brogdon C, Hu L, Masurat T, Pianotti R, Schumann P. Mechanism of action of an antiseptic, anti-odor mouthwash. J Dent Res. 1983;62(6):738-42.
35. Cortelli JR, Barbosa MD, Westphal MA. Halitosis: a review of associated factors and therapeutic approach. Braz Oral Res 2008;22(Spec Iss 1):44-54
36. Shinada K, Ueno M, Konishi C, Takehara S, Yokoyama S, Zaitsu T, Ohnuki M, Clive Wright FA, Kawaguchi Y. Effects of a mouthwash with chlorine dioxide on oral malodor and salivary bacteria: a randomized placebo-controlled 7-day trial. Trials 2010 11:14.
37. Quirynen M, Avontroodt P, Soers C, Zhao H, Pauwels M, Coucke W, van Steenberghe D. The efficacy of amine fluoride/stannous fluoride in the suppression of morning breath odour. J Clin Periodontol 2002; 29: 944-954.
38. Fedorowicz Z, Aljufairi H, Nasser M, Outhouse TL, Pedrazzi V, Mouthrinses for the treatment of halitosis. Cochrane Database Syst Rev. 2008; 8(4):CD006701.
39. Lodhia P, Yaegaki K, Khakbaznejad A, Imai T, Sato T, Tanaka T, Murata T, Kamoda T. Effect of green tea on volatile sulfur compounds in mouth air. J Nutr Sci Vitaminol 2008; 54(1):89-94.
40. Xu X, Zhou XD, Wu CD. Tea Catechin EGCg Suppresses the mgl Gene associated with halitosis. J Dent Res 2010;89 (11):1304-1308
41. Feng X, Chen X, Cheng R, Sun L, Zhang Y, He T. Breath malodor reduction with use of a stannous-containing sodium fluoride dentifrice: A meta-analysis of four randomized and controlled clinical trials. Am J Dent 2010;23 Sp Is B:27B-31B
42. Peruzzo DC, Salvador SL, Sallum AW, Nogueira-Filho GR. Flavoring agents present in a dentifrice can modify volatile sulphur compounds (VSCs) formation in morning bad breath. Braz Oral Res 2008;22(3):252-7 |