Introduction
Tooth rotation, is defined as observable mesiolingual or distolingual intra-alveolar displacement of the tooth around its longitudinal axis. Rotation of teeth can be caused by number of factors like space availability for tooth alignment, tooth eruption order, and functional influences exerted by the tongue and lips consonant with a multifactorial model in the origin of tooth malpositions.1,4 Supernumerary tooth can also cause tooth rotation and mesiodens is the commonest among this anomaly. In addition, mesiodens can delay or prevent eruption of central incisors in 26-52% of cases, cause ectopic eruption, displacement or rotation of a central incisor in 28-63% of cases, and labially displace incisors in 82% of cases
Mesiodens frequently causes retention of permanent incisors which erupt spontaneously after the extraction of supernumerary tooth, if it is conserving the eruptive force and there is sufficient space in the dental arch. Other complications involving the permanent incisors include dilacerations of the developing roots, root resorption and loss of tooth vitality2, 3. Thus, a significant delay in treatment can create the need for more complex surgical and orthodontic management.
The aim of this case report is to introduce a potentially convenient approach as compared to conventional orthodontic procedure for treatment of rotated maxillary central incisor.
Case Report
A 7 ½ -year-old boy was referred to the Department of Pedodontics with rotated left upper permanent central incisor.
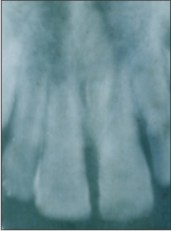
The child's dental history was non-contributory for pertinent findings. The clinical examination showed good facial symmetry and competent lips at rest. Intra oral examination revealed Class I malocclusion with severe rotation of left maxillary central incisor. Radiograph revealed the presence of a mesiodens in the premaxillary region and no associated pathology was seen in the root of central incisor. Shift cone technique confirmed its palatal location. (fig 1)
 | Fig 1 Preoperative Periapical Radiograph
 |
Decision was taken to remove the mesiodens and correct the rotated tooth by means of surgery. An acrylic splint was fabricated with rotated tooth and that region of 21 was hollowed out so that it can be tried before as well as after surgical derotation procedure. Hence, it confirms the occlusal comfort of the patient with the splint before the intended surgery and can immobilize the derotated tooth in a most passive position.
Before surgery the splint was tried inside the mouth to conform the fit and comfort of the patient (fig 2.3). Then the tooth was extracted by raising a palatal flap and cutting the bone without damaging the roots of adjacent central incisors (fig 2.1). Rotated tooth was held by an ideal extraction forceps along with gauge piece for better grip and to prevent the tooth from coming out of its socket (fig 2.2). The tooth was gently luxated within the socket but at the same time, no excess force was given to over rotate. It was turned carefully to the desired position without delivering any pull or push force.
 | Preoperative Study Model
|
 | Fig 2.1 Mesiodens Exposed For Removal
|
 | Fig 2.2 Rotating Incisor With Forceps Held With Gauge
|
Then splint was cemented and kept for 3 weeks (fig 2.4). Patient was followed for 13 months. Periapical radiograph showed normal physiological root development with no signs of infection or root resorption and also there was evident reduction in midline diastema. (fig 3.1,3.2).
 | Fig 2.3 Presurgical Trial Of The Splint
|
 | Fig 2.4 Postsurgical Placement Of The Splint
|
 | Fig 3.1 Post Operative Radiograph
|
Discussion
Conventional treatment of rotation is generally done by fixed or removable appliance but both these procedures have their inherent disadvantages. If a fixed appliance had to be given in this case, we would have to wait for root completion, and removable appliance may not give the desired result.
Disadvantages and potential risks of orthodontic treatment
1) Decalcification- The presence of a fixed appliance predisposes to plaque accumulation as tooth cleaning around the components of the appliance is more difficult. Decalcification during treatment with fixed appliances is a real risk, with a reported prevalence of between 2 and 96 per cent.
2) Loss of periodontal support-As a result of reduced access for cleansing, an increase in gingival inflammation is commonly seen following the placement of fixed appliances. Removable appliances may also be associated with gingival inflammation, particularly of the palatal tissues, in the presence of poor oral hygiene.
3) Root resorption-It is now accepted that some root resorption is inevitable as a consequence of tooth movement. On an average, during the course of a conventional 2-year fixed-appliance treatment around 1 mm of root length is lost.
4) It is usually said, rotations are easy to treat, but very difficult to retain1. They have a very high risk of relapse due to stretching of the supra-alveolar and transeptal gingival fibers which readapt very slowly to the new position. Thus long term retention is required to achieve stability of treatment.
Advantages of "surgical derotation" are:
a) Duration of treatment is short
b) Retention is not required
c) Patient cooperation is less critical
Reasons for selecting this approach in this case were 1) age of the patient 2) tooth was in erupting stage 3) root was with wide open apex 4) enough space was present for accommodation of derotated tooth and 5) shape of the root of central incisor was round.
Use of the acrylic splint described here offers the following advantages: (1) maximum patient comfort, (2) good occlusion and mastication, (3) ease of insertion, (4) easy readjustment, if needed, and (5) maximum stability8.
Even though, during derotation damage to periodontal ligament is inevitable, according to American Academy of Endodontics if tooth is reimplanted within the first 5 min, root surface fibroblasts and precursor cells from the root and alveolar periodontal ligament can live, reproduce, and become functional fibroblasts, capable of producing a united periodontal ligament to protect the root from resorption.5,6
A frequent justification for early intervention is that it can reduce the severity and complexity of comprehensive treatment with fixed appliances. The goal of early treatment is to establish normalcy for further growth and development. This, in turn, allows us to maximize positive growth patterns and to minimize distalization mechanics in treatment.
Conclusion
Surgical derotation or intentional derotation can be used for treatment of rotated tooth but ideal case selection and judicious surgical approach is mandatory for desired results.
References
1. St. Louis, Proffit, W.R., Fields, J.R.,. Contemporary Orthodontics, third ed. Mosby Co.2000; pp 124-127.
2. Giancotti, A., Grazzini, F., De Dominicis, F., Romanini, G., Arcuri, C.,. Multidisciplinary evaluation and clinical management of mesiodens. J. Clin. Pediatr. Dent 2002;26:233 -238.
3. Gundu z, K., Mug¢lali, M.,. Non-syndrome multiple supernumerary teeth: a case report. J. Contemp. Dent. Pract 2007;8: 81-87.
4. Baccetti, T.,. Tooth rotation associated with aplasia of nonadjacent teeth. Angle Orthod. 1998;68: 471-474.
5. Arezoo Jahanbin, Bahareh Baghaii, Iman Parisay,. Correction of a severely rotated maxillary central incisor with the Whip device. The Saudi Dental Journal 2010;22: 41-44.
6. Kudou Y, Kubota M.. Replantation with intentional rotation of a complete vertically fractured root using adhesive resin cement. Dent Traumatol 2003;19: 115-117
7. Priyanka Rai, Udayan Gupta, Namita Kalra. Self-replantation of an avulsed tooth in torsoversion: a 10 - year follow-up. Dent Traumatol 2007;23:158-161
8. Glenn M. Biven, Major, DC; USA, Gary M. Ritchie Major, DC; USA and Harold Gerstein B.S., D.D.S. Acrylic splint for intentional replantation. Oral Surgery, Oral Medicine, Oral Pathology 2005;30(4): 537-539 |