Introduction
Cemento-ossifying fibroma (COF) is a fibro-osseous lesion that arises from the periodontal membrane.1 The periodontal membrane is a layer of fibrous connective tissue surrounding the roots of teeth. It contains multipotential cells that are capable of forming cementum, lamellar bone, and fibrous tissue.2, 3 Although central COFs of the mandible are common, they are infrequent in the maxilla.4
This lesion should be distinguished from fibrous dysplasia of bone and certain other fibro-osseous lesions that do not represent true neoplasia.5 A close histogenetic relationship exists between the central COF and the central ossifying fibroma. The pathologic differences between central COF and fibrous dysplasia are few and the diagnosis must be made in light of the radiographic findings.6
Case Report
A 40-year-old male patient reported with a chief complaint of a painless swelling in the upper front region for a period of 3 years. Initially, the swelling was small in size and showed a gradual increase to its present dimensions. Extra oral examination showed a diffuse swelling in the upper front region (Fig 1).
 | Fig 1: 40-year-old Male Patient With An Enlargement In The Maxillary Anterior Region.
 |
The skin over the swelling was normal, and there was no local rise of temperature. On palpation the swelling had variable consistency. Buccal cortices were expanded. The lesion was smooth, non tender and hard; there was no accompanying cervical lymphadenopathy
The physical examination revealed a maxillary enlargement and an intraoral lesion. The teeth were agile and displaced. The swelling extended from 11 to 22 and it obliterated the buccal vestibule (Fig 2). Oral mucosa was normal. The overlying mucosa
 | Fig 2: Firm Mass Of Size 4 X 4 Cm Extending From 11 To 22 Which Had Almost Effaced The Jugogingival Groove. The Teeth Were Agile And Displaced.
|
was reddish pink in color and slightly swollen but there was no ulceration or fistula formation. On palpation, the swelling was bony hard in consistency but no tenderness or paraesthesia. His medical history was not contributory and physical examination disclosed no evidence of any systemic disease. No history of trauma to the maxilla could be elicited.
Radiographically, orthopantomograph, occlusal & intra oral periapical radiograph (Fig 3, 4, 5) showed a well-defined large multilocular radiolucent lesion (approx 4x4 cm) extending from 11 to 22. The lesion was well demarcated with sclerotic border and heterogeneous in contrast. The mass did not invade the maxillary sinus. No evidence of cortical erosion was noticed. The radiographic differential diagnosis included odontogenic myxoma, COF, fibrous dysplasia (FD), focal cemento-osseous dysplasia (FCOD), desmoplastic ameloblastoma and central giant cell granuloma.
 | Fig 3: Orthopantomograph Showing A Well-defined Multilocular Lesion With Radiolucent And Radio-opaque Foci.
|
 | Fig 4: Occlusal Radiograph Showing The Extent Of The Lesion (approx 4 X 4 Cm) That Contained Small Foci Of Calcification Extending From The 11 To 22.
|
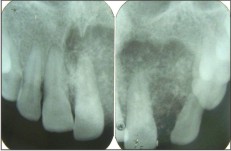 | Fig 5: Intraoral Periapical Radiographs Showing The Extent Of The Lesion (approx 4 X 4 Cm) That Contained Small Foci Of Calcification Extending From The 11 To 22.
|
A biopsy was performed under local anaesthesia and the specimen was sent for histopathology examination. Histopathological examination showed stratified squamous epithelium where deeper areas showed intense fibroblastic proliferation with calcifications of different sizes and shapes. Bony trabeculae rimmed by osteoblasts were seen . The patient's medical history did not reveal any pathological condition. Therefore, surgical excision of the lesion was proposed to the patient.
Management
The surgical intervention was carried out in the Department of Oral and Maxillofacial Surgery. Wide surgical excision of the lesion was subsequently performed (Fig 6) and the tissue was sent for histopathological examination (Fig 7).
 | Fig 6: The Surgical Specimen (gross Appearance)
|
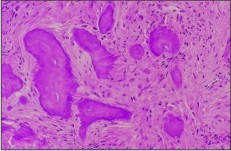 | Fig 7: Histopathologically Deeper Areas Showed Intense Fibroblastic Proliferation With Calcifications Of Different Sizes And Shapes. Bony Trabeculae Rimmed By Osteoblasts Were Seen.
|
The clinical, radiographic and histologic findings were consistent with COF. The postoperative course was uncomplicated and there was no lesion recurrence up to one year of follow-up.
Discussion
COF is generally classified as a type of fibro-osseous lesion of the jaws. The mandible is more commonly involved than the maxilla, and the premolar-molar region is the most common site. Small lesions are often symptomless. Large lesions result in painless swelling of the involved bone which may cause obvious facial asymmetry.7 In some cases, initial symptoms are present.8
The radiographic appearance depends on the location and the amount of calcified tissue present. Varying degrees of radiopacities and radiolucencies may be present. Central COFs are typically well-defined, solitary radiolucencies with scattered radiopaque foci. They maintain a spherical shape, expand cortical bone without causing perforation, and may cause tooth divergence.9 The central COF, have a centrifugal growth pattern rather than a linear one. Therefore the lesion grows by expansion equally in all directions and present as round tumor mass.
Generally, COF characterised by a well-defined expansile bony mass and rarely associated with destruction or extraosseous soft tissue components.10 Unlike the COF, the aggressive cemento-ossifying fibroma (ACOF) grows massively with extensive cortical expansion.9, 11 There are no histopathologic criteria that are predictive of aggressive behaviour or tendency for recurrence. Nevertheless, Zupi et al. reported two features that may help in distinguishing ACOF from COF. Firstly, clinically, the ACOF occurs at a far lower mean age than the COF. Secondly, the histological pattern of the ACOF seems to be unique in being highly cellular with entrapped osteoblasts. However, considering the age, radiographic appearance and the growth behaviour, our case would clearly fit under the COF category, the non-aggressive type.
COF is a slow-growing lesion composed of cellular fibroblastic tissue containing basophilic masses of cementum-like tissue. In addition, varying amounts of bony trabeculae are interspersed within the lesion, giving it its characteristic features 6, 12 used the presence or absence of woven and lamellar bone in histopathological section to differentiate the COF from the other fibro-osseous lesions. In uncomplicated cases, fibrous dysplasia contains no lamellar bone but, rather, has arrested woven bone. On the other hand COF and ossifying fibroma contain woven bone and are often rimmed by osteoblasts that have laid down layers of lamellar bone. Additionally COF may have areas of cementum, appearing as psammoma bodies embedded in a benign fibrous stroma.
Large tumors may involve the nasal septum, orbital floor, and infraorbital foramen. The tumor extent guides surgical therapy. Maxillary central COFs are large at the time of presentation, indicating the capacity of the tumor to expand freely within the maxillary sinus. Pathologic examination of the central COF shows a proliferation of irregularly shaped calcifications within a hypercellular fibrous connective tissue stroma. The calcifications are extremely variable in appearance and represent various stages of bone and cementum deposition. The circumscribed nature of the lesion permits complete local enucleation or curettage of small lesions. Large lesions that have destroyed a considerable amount of bone may require segmental resection and reconstruction.
References
1. Huebner GR, Brenneise CV, Ballenger J. Central ossifying fibroma of the anterior Maxilla: Report of case. J Am Dent Assoc 1988;116:507-10.
2. Bertrand B, Eloy P, Cornelis JP, Gosseye S, Clotuche J, Gilliard C. Juvenile aggressive cement-ossifying fibroma: Case report and review of the literature. Laryngoscope 1993;103:1385-90.
3. Hamner JE 3 rd, Lightbody PM, Ketcham AS, Swerdlow H. Cemento-ossifying fibroma of the maxilla. Oral Surg Oral Med Oral Pathol 1968; 26:579-87.
4. Sarita M, Raj KA, Daya SM, Rohtas KY. Cemento-ossifying Fibroma of the Maxilla. Indian J Radiol Image 2000;10:103-4.
5. Waldron CA, Giansanti JS. Benign fibro-osseous lesions of the jaw: A clinical-radiologic-histologic review of 65 cases. Oral Surg Oral Med Oral Pathol 1973;35:190-201.
6. Kuta AJ, Worley CM, Kaugars GE. Central Cemento-ossifying fibroma of the Maxillary sinus: A review of six cases. AJNR Am J Neuroradiol 1995;16:1282-6.
7. Hwang EH, Kim HW, Kim KD, Lee SR. Multiple cemento-ossifying fibroma: report of an 18-year followup. Dentomaxillofac Radiol. 2001; 30:230-4.
8. Su L, Weathers DR, Waldron CA Distinguishing features of focal cemento-osseous dysplasias and cemento-ossifying fibromas: I. A pathologic spectrum of 316 cases. Oral Surg Oral Med Oral pathol Oral Radiol Endod. 1997; 84:301-9.
9. Montgomery AH. Ossifying fibroma of the jaw. Arch Surg 1938;36:874-98.
10. Jung SL, Choi KH, Park YH, Song HC, Kwon MS. Cemento-ossifying fibroma presenting as a mass of the parapharyngeal and masticator space. AJNR Am J Neuroradiol. 1999; 20:1744-6.
11. Zupi A, Ruggiero AM, Insabato L, Senghore N, Califano L. Aggressive cemento-ossifying fibroma of the jaws. Oral Oncol. 2000; 36:129-33.
12. Reed RJ. Fibrous dysplasia of bone: A review of 25 cases. Arch Pathol 1963;75:480-95. |