|
|
|
| Intraosseous Calcifying Epithelial Odontogenic Tumor - A Case Report |
Sumit Chopra 1 , Pawan Arora 2 , Rakhi Gupta 3 , Sucheta Bansal 4
1 MDS, Reader, Department of Oral and Maxillofacial Pathology - Himachal Institute of Dental Sciences, Paonta Sahib
2 Professor, Department Of Pedodontics - Sarabha Dental College, Ludhiana
3 MDS (Reader), Deptt. of Oral Pathology & Microbiology - Himachal Institute of Dental Sciences,Paonta Sahib (H.P.). PIN-124001
4 MDS, Sr. Lecturer, Department of Oral and Maxillofacial Pathology - Himachal Institute of Dental Sciences, Paonta Sahib
|
| Address For Correspondence |
Dr. Sumit Chopra, MDS, Reader
Dept. Of Oral And Maxillofacial Surgery
Himachal Institute Of Dental Sciences, Paonta Sahib. |
| Abstract |
| Odontogenic tumors constitute a group of heterogeneous disease derived from epithelial, mesenchymal and/or ectomesenchymal elements. The CEOT is a benign, though occasional locally invasive, slow-growing neoplasm occurring as intraosseous (94%) and extraosseous (6%) variants. CEOT shows a relative frequency of 1-2%. The extraosseous variant is diagnosed slightly earlier (mean age 34.4 years) than the intraosseous type (mean age 38.9 years). Both variants have an almost 1:1 gender ratio. The intraosseous CEOT shows a maxilla:mandible site ratio of 1:2 and are mainly located in the premolar/molar region. CEOT originates from the complex system of dental laminae or remnants thereof. Histologically, the CEOT is characterized by the occurrence of sheets, nests and masses of polyhedral, eosinophilic epithelial cells which may show cellular abnormalities including giant cell formation and nuclear pleomorphism. Some cells increase in size and produce a homogeneous, eosinophilic, 'amyloid-like' substance which may become calcified and which may be liberated as the cells break down. |
|
| Keywords |
| TUMOUR, CALCIFICATION, ODONTOMA EPITHELIUM PINDBORG |
|
| Full Text |
Introduction
The calcifying epithelial odontogenic tumor is a benign odontogenic tumor of epithelial origin that accounts for approximately 1% of all odontogenic tumors[1]. The calcifying epithelial odontogenic tumour was first described as a distinct entity by Pindborg (1958)[2]. The origin of this neoplasm is not clearly known, although it is generally accepted to be derived from oral epithelium, reduced enamel epithelium, stratum intermedium or dental lamina remnants[1]. Evans (1966)[3] has suggested that the tumour is a variant of ameloblastoma, but, as Abrams and Howell (1967)[4] have pointed out the calcifying epithelial odontogenic tumour differs from it by having no preameloblasts or stellate reticulum.
In the ultrastructural study done by Anderson, Kim, and Minkowitz (1969) the tumour cells showed features which were commonly seen in epidermal cells in accordance with origin from the enamel organ or oral epithelium.[5]
It is more common in the posterior part of the mandible of adults in the fourth to fifth decades. There is no gender predilection. It is characterized by squamous epithelial cells, calcifying masses, and homogeneous acellular material admixed with the tumor epithelium and stroma that have been identified as amyloid.[6]
In this article we are presenting a case report of an elderly female patient having tumor on right side of maxilla.
CASE REPORT
A patient 60yrs female, reported to our department with the chief complaint of swelling on right upper back teeth region since 1month. Swelling was progressively increasing in size and was painful from the last 15-20 days. There was mild pain and associated white watery discharge intra orally from the swelling on pressure application. Patient gave history of extraction with respect to posterior teeth around 20 yrs. back.
Extraoral examination showed facial asymmetry and a bony hard swelling on the upper right back tooth region.
Intra oral examination revealed an ovoid, bony hard swelling which was non-tender on palpation. Overlying surface was normal with ulceration at one point. Patient is completely edentulous.
On aspiration, needle entered the tissue but did not aspirate anything.
Radiographic investigations included OPG and CT scan. OPG well defined radiolucent lesion with multiple foci. CT scan revealed large expansile bony lesion arising likely from alveolar process of maxilla (Fig 1).
 | Fig.1 OPG showing well defined radiolucent lesion with multiple foci on right maxilla.
 |
An incisional biopsy was performed and microscopic examination revealed proliferation of polyhedral shaped epithelial cells with eosinophilic cytoplasm which demonstrated mildly nuclear pleomorphism. We observed calcifications which were in the form of Liesegang rings.
DISCUSSION
The calcifying epithelial odontogenic tumor, also known as a Pindborg tumor or CEOT, is an odontogenic tumor first recognized by the Dutch pathologist Jens Jorgen Pindborg in 1955. It was previously described as an adenoid adamtoblastoma, unusual ameloblastoma and acystic odontoma. Like other odontogenic neoplasms, it is thought to arise from the epithelial element of the enamel origin namely epithelial rests of dental lamina or reduced enamel epithelium.[7]
It is a benign, slow growing, but invasive neoplasm. The incidence of calcifying epithelial odontogenic tumor is only 1%. It is more common in the posterior mandible of adults[8], typically in the 4th to 5th decades. There is no sex predilection but it is more common in whites. It appears clinically to be a slowly enlarging painless mass. In the maxilla it can cause proptosis, epistaxis and nasal air way obstruction. Its recurrence rate is 10-15%.[9] Franklin and Pindborg reported a recurrence rate of 14%.[10] It is considered to have a recurrence rate much lower than the recurrence rate for ameloblastoma.[7]
It has two types: Intraosseous ceot and extraosseos ceot. The intraosseous type appears radiographically as an irregular, uni- or multilocular radiolucent area containing radiopaque masses which increases in size and opacity with time. Some 60% of intraosseous CEOT are associated with an unerupted tooth (or odontoma). CEOT shows a relative frequency of 1-2%. The extraosseous variant is diagnosed slightly earlier (mean age 34.4 years) than the intraosseous type (mean age 38.9 years). Both variants have an almost 1:1 gender ratio.[8]
Radiographically, these lesions can be radiolucent, but they more characteristically are mixed lucent and opaque masses, exhibiting a snow-driven appearance.
Histologically, the CEOT or Pindborg tumor is composed of polyhedral epithelial cells with scanty stroma. The closely packed cells demonstrate nuclear pleomorphism. Variable amounts of an homogenous material is seen. This has been shown to be amyloid or a similar substance. [11,12,13] However, calcification is an important feature and sometimes it cannot be seen. In some cases clear cell nests may be observed.[8,11,14,15] The first two features are necessary for the diagnosis. We observed, especially in the peripheral areas of the tumor, the polyhedral shaped cells with eosinophilic cytoplasm which demonstrated mildly nuclear pleomorphism (Fig. 2).
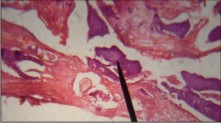 | Fig2. Showing proliferation of polyhedral shaped epithelial cells in the form of sheets. Calcifications are also seen.
|
We observed calcifications in the form of Liesegang rings.
Histological variants including CEOT with cementum-like components, clear-cell CEOT (15 cases reported so far), CEOT-containing Langerhans' cells, combined epithelial odontogenic tumour (CEOT/AOT) and CEOT with myoepithelial cells.[12]
The treatment of this lesion is complete surgical excision. The recurrence rate for CEOT is 4%. The lesion is slow growing and requires long-term follow-up monitoring for recurrence (at least 5-10 y). No cases of malignant transformation are reported.
References
1. Deboni MC et al. Clinical, radiological and histological features of calcifying epithelial odontogenic tumor: Case report. Braz Dent J 2006;17:171-4
2. Pindborg, JJ. A calcifying epithelial odontogenic tumor. Cancer (Philad.), 1958,11;838-843.
3. Evans, RW. Histological Appearances of Tumours, 2nd ed.1966, p. 972. Livingstone, Edinburgh.
4. Abrams, AM, Howell, FV. Calcifying epithelial odontogenic tumors; report of four cases. J. Amer. dent. Ass., 1967,74:1231-1240.
5. Anderson HC, Kim B, Minkowitz S. Calcifying epithelial odontogenic tumor of Pindborg. An electron microscopic study. Cancer (Philad.),1969, 24:585-596.
6. Dabir A, Padhye M. Calcifying epithelial odontogenic tumor - A case report. (Pindborg's Tumor). Scientific Journal Vol. II - 2008.
7. Ida Marie Tabangay-Lim, Raymund Noel C. Mallari, Noelito M. Lacsamana et al. "Recurrent calcifying epithelial odontogenic tumor (Pindborg tumor): A case study". Oral Oncology, 2005;41(10):259-266.
8. Philipsen HP, Reichart PA. "Calcifying epithelial odontogenic tumour: biological profile based on 181 cases from the literature." Oral Oncol, 2000;36(1):17-26.
9. Anderson's pathology (10 ed.). Mosby. 1996. pp. 1603-1604.
10. Franklin CD, Pindborg JJ. "The calcifying epithelial odontogenic tumor. A review and analysis of 113 cases.". Oral Surg Oral Med Oral Pathol, 1976;42(6):753-65.
11. Pilch BZ. Head and neck surgical pathology. Lippincott Williams and Wilkins: Philadelphia 2001.
12. Philipsen HP, Reichart PA, Nikai H, Takata T, Kudo Y. Peripheral ameloblastoma: biologic profile based on 160 cases from the literature Oral Oncol 2001;37:17-27.
13. Murphy CL, Kestler DP, Foster JS, Wang S, Macy SD, Kennel SJ et al. Odontogenic ameloblast-associated protein nature of the amyloid found in calcifying epithelial odontogenic tumors and unerupted toothe follicules. Amyloid 2008;15:89-95.
14. Takata T, Ogawa I, Myauchi M, Ijuhin N, Nikai H, Fujita M. Noncalcifying Pindborg tumor with langerhans cells. J Oral pathol Med 1993;22:373-83.
15. Gunhan O, Erseven G, Ruacan S, Celasun B, Aydintug Y, Ergun E, Demiriz M. Odontogenic tumors. A series of 409 cases. Aust Dent J 1990;35:518-22. |
|
|
|
|
|
|