|
|
|
| One-stage Surgical Alveolar Augmentation (paoo) For Rapid Orthodontic Movement. A Case Report. |
Ashish Jain 1 , Tarun Das 2 , Rashi Chaturvedi 3
1 MDS, Professor and Head, Dept. Of Periodontics - Dr. H.S.J. Institute Of Dental Sciences And Hospital Panjab University, Chandigarh
2 MDS, Senior Lecturer, Dept. Of Periodontics - Dr. H.S.J. Institute Of Dental Sciences And Hospital Panjab University, Chandigarh
3 M.D.S, D.N.B, Reader, Dept. Of Periodontics - Dr. H.S.J. Institute Of Dental Sciences And Hospital Panjab University, Chandigarh
|
| Address For Correspondence |
Dr.Tarun Das
Address: House no.1036/2,
Sector 40B, Chandigarh-160036
Contact: + 91-986602872
E-mail: tarundas13@yahoo.com |
| Abstract |
| Abstract
Corticotomy found to be effective in accelerating orthodontic treatment. Corticotomy facilitated orthodontics advocated for comprehensive fixed orthodontic appliances in conjunction with full thickness flaps and labial and lingual corticotomies around teeth to be moved. Bone graft should be applied directly over the bone cuts and the flap sutured in place. Tooth movement should be initiated two weeks after the surgery, and every two weeks thereafter by activation of the orthodontic appliance. Orthodontic treatment time with this technique will be reduced to one-third the time of conventional orthodontics. Alveolar augmentation or labial and lingual cortical plates were used in an effort to enhance and strengthen the periodontium, reasoning that the addition of bone to alveolar housing of the teeth, using modern bone grafting techniques, ensures root coverage as the dental arch expanded. Corticotomy facilitated orthodontics is promising procedure but only few cases were reported in the literature. The case report highlights the PAOO technique and the treatment of a 24 year old male. |
|
| Keywords |
| Corticotomy facilitated orthodontics; Rapid orthodontics; Accelerated osteogenic orthodontics; Regional acceleratory phenomena; Periodontally accelerated osteogenic orthodontics |
|
| Full Text |
Introduction
An increasing number of adult patients have been seeking orthodontic treatment, and a short treatment time has been a recurring request. As result a number of surgical techniques have been developed because the surgical injury of the cortical bone adjacent to the area of desired tooth movement has been reported to initiate biochemical changes leading to rapid tooth movement[1].
Wilcko et al. introduced surgical orthodontic therapy which included the innovative strategy of combining corticotomy surgery with alveolar grafting in a technique referred to as Accelerated Osteogenic Orthodontics (AOO) and more recently to as Periodontally Accelerated Osteogenic Orthodontics (PAOO)[2-5]. Significant acceleration in orthodontic tooth movement has been extensively reported following a combination of selective alveolar decortication and bone grafting surgery, with the latter being responsible for the increased scope of tooth movement and the long-term improvement of the periodontium. This conventional corticotomy approach consists of raising full-thickness flaps and using a bur to create cortical incisions. Then an allograft is placed at the sites needing the bone expansion necessary for proper orthodontic tooth movement. This intentional injury to the cortical bone results in a modification of the bone metabolism, leading to a transient state of osteopenia, described as rapid acceleratory phenomenon (RAP). RAP was demonstrated at the alveolar bone level following corticotomy and would be responsible for rapid tooth movement.
Case Description
A 24-year-old male was referred to orthodontic consultation for deep bite and retro-positioned lower incisors which were not allowing maintenance of oral hygiene in the lingual aspect of the lower incisors and attrition of the lower incisors. He strongly expressed the demand for a rapid completion of her treatment, citing professional and personal reasons. His dental history included regular dental visits and complete oral prophylaxsis.
Extraoral and intraoral examination
The patient showed a symmetrical face and a normal soft-tissue profile with normal vertical facial height (Figure1a-c).
 | Figure 1a-c
 |
The temporomandibular joints were within normal limits. The lips were competent at rest with adequate vermillion display. Patient presented with a class I molar and canine relationship. The incisors presented with relationship similar to that of seen class II division 2 relationship. The overjet was 0mm, and the overbite was ~100% of lower incisor coverage.When smiling, he exhibited 100% of maxillary incisal display. The maxillary dental midline was coincident with the facial midline and maxillomandibular midlines were concordant (Figure 1d-f).
 | Figure 1d-f
|
The maxillary and mandibular arch forms were U-shaped maxillary arch had 3mm of crowding while mandibular arch presented 6 mm of crowding with few rotated teeth (Figure 2a,b).
 | Figure 2a-b
|
The curve of Spee was 3 mm, and the periodontium was healthy.
From a skeletal standpoint, he had a class I pattern with normal lengths maxilla and mandible, a hypodivergent mandible, reduced lower anterior facial height and retroclined upper and lower incisors.
Treatment Objectives
The goal of the treatment was to resolve the crowding in both arches, open the bite, to correct the incisor relations and maintain class I dental relationship that would be pleasing to the patient and decrease treatment duration. The patient was offered the conventional orthodontic treatment as well as an innovative treatment combining comprehensive orthodontic care with periodontal surgery (PAOO) to accelerate tooth movement. In this procedure, a bone graft was also planned in the area where expansion was needed to expand the bony envelop in the direction of tooth movement and increase periodontal support to improve long-term stability in areas where relapse commonly occurs following orthodontic expansion. Because the patient sought a short treatment time, the orthodontic treatment coupled with PAOO was chosen.
Surgical Technique
The fixed orthodontic appliance (Gemini 22 slot brackets, MBT prescription, 3M) was placed with standard technique onto the upper arch only, consisting of second premolar to second premolar brackets and bands with buccal tubes on 1st molars. Alignment and leveling was initiated with round NiTi wires. The surgery was performed 2 week following placement of the fixed orthodontic appliance.
On the day of surgery, orthodontic archwire was removed and patient was asked to perform mouth-brushing. 2grams of amoxicillin was taken by the patient 30 minutes prior to the surgery. On the dental chair chlorhexidine mouthwash was performed by the patient. After local anesthesia, full thickness buccal flap was raised from mesial of 15 to mesial of 25 with crevicular incisons maintaining the interdental papillae. Vertical release incisions were performed inter-proximally between 14-15 & 24-25 (Figure 3a).
 | Figure 3a-d
|
Bony prominences on the canine roots were leveled with help of straight diamond burrs. Corticotomy was done on the exposed bone surface with help of round diamond burrs mounted on a reduction mircomotor hand-piece under copious amount of irrigation (Figure 3b, c).
Demineralized freeze-dried bone allograft was mixed with saline and formed into a thick paste. The graft was packed onto the modified bone surface (Figure 3d).
Flaps were positioned and sutured with silk sutures (Figure 4).
 | Figure 4
|
Orthodontic archwire was secured back into the brackets.
Patient was instructed to apply local cold fomentation intermittently for first 12 hours after the surgery. He was also instructed to only take cold diet for 24 hours. Amoxicillin coverage was to continue for 3 more days. Rigorous brushing in the area of surgery was advised against for the 1st week. Check up was scheduled for the next day.
Treatment Progress
The patient reported using only two tablets of the NSAID after surgery. No swelling, bruising, or severe discomfort was associated with this procedure. The patient could resume oral physiotherapy 24 hours after the surgery. The periodontal healing was optimum with minimal to no scarring at 2 weeks.
During the first 6 to 10 weeks of orthodontic treatment, the maxillary arch was fully leveled and aligned using increasing size of nickel titanium alloy wires (0.014, 0.016, 0.018, 0.016 x 0.022). Bite opening and arch expansion was achieved with reverse curved stainless steel wire and stoppard steel wire.
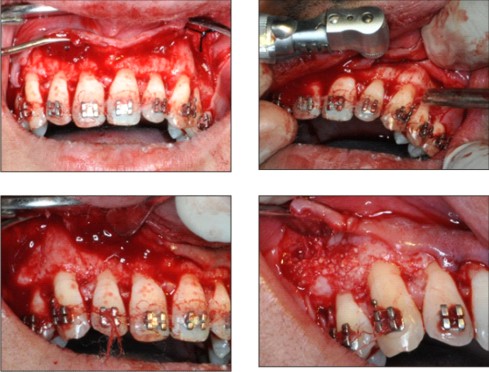
In the following six weeks adequate maxillary arch expansion and bite opening was achieved so as to allow the bonding of the mandibular arch. 2 weeks following the bonding of the mandibular arch corticotomy surgery was planned and executed in a manner similar to that of the maxillary arch. The only differences was that the mandibular archwire was not removed from the bracket as there ease of excess to the anterior alveolus (Figure 5a-c, Figure 6).
 | Figure 5a-c
|
 | Figure 6
|
During the course of treatment (figure 7),
 | Figure 7
|
a sharp increase in tooth mobility was observed, resulting from the transient osteopenia induced by the surgery. Also important to emphasize is that higher forces are applied to the teeth as compared with conventional orthodontic treatment to maintain mechanical stimulation of the alveolar bone and the osteopenic state, allowing for rapid treatment.
Treatment Results
After 26 weeks of active treatment, sequential de-bonding was performed. The brackets on the premolars were removed to allow them settle into occlusion. 4 weeks later complete appliance was removed and a fixed lingual retainer was inserted from premolar to premolar on both arches. To maintain the bite, circumferential retainer with anterior bite plane was given to the patient to be worn 24 hours (figure 8a-e).
 | Figure 8a-e
|
Comments
It is of paramount importance for the orthodontist and surgeon to understand that the surgically induced high tissue turnover is restricted to the immediate proximity of the surgical cuts creating what might be referred to as a localized spatio-temporal window of opportunity. Attention must be given to perform the bony incisions only around the teeth where tooth movement is planned. As such, the relative anchorage value of the teeth away from the surgical site remains high and anchorage value of teeth adjacent to the surgical site is low. Rapid acceleratory phenomenon (RAP) is transient, but continuous mechanical stimulation of the teeth would prolong the osteopenic effect induced by the procedure. Hence, it is imperative to see the patient and adjust the orthodontic appliance every 2 weeks.
Conclusions
PAOO is an innovative, technique to achieve rapid orthodontic tooth movement. This novel technique also allows the possibility for hard- and/or soft-tissue augmentation, leading to an enhanced periodontium and an increased scope of tooth movement. PAOO proves to be efficient from both the patients' and clinicians' standpoints and offers the advantages that should lead to greater acceptance in the dental community.
References:
1. Bogoch E, Gschwend N, Rahn B, et al. Healing of cancellous bone osteotomy in rabbits-part I: regulation of bone volume and the regional acceleratory phenomenon in normal bone. J Orthop Res. 1993;11(2):285-291.
2. Wilcko, M.T., Wilko, W.M., Bissada, N.F., 2008. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: a synthesis of scientific perspective. Seminars Orthod. 14: 305-316.
3. Wilcko, M.W., Ferguson, OJ" Bouquot. J.E., Wilcko, M.T., 2003. Rapid orthodontic decrowding with alveolar augmentation: case report. World J. Orthod. 4. 197-205.
4. Wilcko, W.M., Wilcko, M.T., Bouquot. J.E., Ferguson, OJ., 2000. Accelerated orthodontics with alveolar reshaping. J. Ortho. Practice 10, 63-70.
5. Wilcko, W.M., Wilcko, T., Bouquot, J.E., Ferguson, OJ., 2001. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int. J. Periodont. Restorat. Dent. 21. 9-19 |
|
|
|
|
|
|