Introduction
Mineral trioxide aggregate (MTA) was developed at Loma Linda University in the 1990s as a root-end filling material. MTA was first described in the dental scientific literature in 1993 1 and was given approval for endodontic use by the U.S. Food and Drug Administration in 1998.2 It received acceptance by the US Federal Drug Administration and is commercially available as ProRoot MTA (Tulsa Dental Products,Tulsa,OK, USA). Two commercial forms of MTA are available (ProRoot MTA) as the grey (GMTA) and white forms (WMTA) and MTA-Angelus (Angelus, Londrina,PR,Brazil) is without calcium sulphate.MTA consists of 50%-75% calcium oxide and 15-25% silicon dioxide, these two together form70-95%of the total mix Investigations have found that lower amounts of iron, aluminum, and magnesium are present in white MTA than in grey MTA. MTA material when mixed produce tricalcium silicate(CaO)3SiO2, tricalcium aluminate(CaO)3.AlO3, Di Calcium silicate(CaO)2SiO2,Tetra calcium alumino ferrite(CaO)4. MTA also contians Al2O3.Fe2O3 Gypsum CaSO4.2H2O, bismuth oxide, and trace amounts of SiO2, CaO, MgO, K2SO4, and Na2SO4 3-5. Hydration of the powder results in a colloidal gel composed of calcium oxide crystals in an amorphous structure: 33% calcium, 49% phosphate, 6% silica, 3% chloride and 2% carbon. This gel solidifies into a hard structure in less than three hours6. Mineral trioxide aggregate (MTA) was developed and recommended initially as a root-end filling material and subsequently has been used for pulp capping, pulpotomy, apexogenesis, apical barrier formation in teeth with open apices, repair of root perforations, and as a root canal filling material. Ideally a root end filling material should be nontoxic, non-carcinogenic, non-genotoxic, biocompatible, insoluble in tissue fluids, and dimensionally stable. MTA is a bioactive material7 that promotes hard tissue formation8and is biocompatible. The first MTA material was described as a fine hydrophilic powder composed predominantly of calcium and phosphorus ions, with added bismuth oxide to provide radiopacity greater than dentin9. The MTA product powder is mixed with supplied sterile water in a 3:1 powder/liquid ratio and it is recommended that a moist cotton pellet be temporarily placed in direct contact with the material and left until a follow-up appointment. Upon hydration, MTA forms a colloidal gel that solidifies to a hard structure in approximately 3-4 hrs 5, 9 with moisture from the surrounding tissues purportedly assisting the setting reaction1. Hydrated MTA products have an initial pH of 10.2, which rises to 12.5 three hours after mixing 4, 9. The setting process is described as a hydration reaction of tricalcium silicate (3CaO·SiO2) and dicalcium silicate (2CaO·SiO2), which is said to be responsible for the development of material strength5. It has a compressive strength equal to zinc oxide eugenol with polymer reinforcement (Caulk IRM Intermediate Restorative Material, Dentsply,York, Pa.) and all-purpose lining and cement (SuperEBA, Harry J. Bosworth, Skokie, Ill.) but less than that of silver amalgam. It is available commercially as ProRoot MTA (Dentsply Tulsa Dental, Tulsa, Okla) and has been advocated for use in vital pulp therapy.10-14
Case Reportc (Case -1)
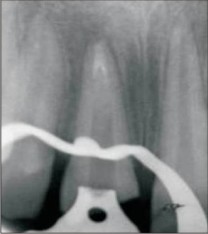
A 26 year male patient reported to department of conservative dentistry and endodontics, Darshan Dental College & Hospital, Udaipur with history of fracture and discoloured tooth #21. Patient gave history of fracture at the age of 7 or 8 years and gave no history of pain or swelling, radiographic examination revealed fractured tooth with open apex and no periapical changes (fig1).
It was decided to seal the open apex with MTA and obturate the root canal. Access opening was made, the working length was estimated and the canals prepared to obtain smooth canal walls. The apex was sealed to about 4mm using MTA (fig 2).
Wet sterile paper point was placed in the canal and temporary restoration was placed. Patient was recalled the following day for obturation. Custom made gutta-percha cone was made and the canal was obturated using lateral condensation technique (fig 3).
Patient was recalled after 6 months an evaluated for prognosis (fig 4).
Six months follow up of case showed hard tissue formation at apex indicating good prognosis.
Case -2
A 25 year old male patient reported to department of conservative dentistry and endodontics Darshan Dental College & Hospital, Udaipur with fractured and discoloured tooth # 21. Patient complained of fractured tooth, pain, swelling and pus discharge. Patient gave history of fall in childhood, patient does not remember the exact age. Patient gave history of swelling and pus discharge since one month. Radiographic examination revealed periapical changes (fig-1a).
Access opening was done and drainage established .The canal was irrigated with normal saline and calcium hydroxide was placed as dressing, after 3 dressings the apex was closed using MTA(fig-2b)
and canal obturated with custom made gutta-percha cone using lateral condensation technique(fig-3c).
Patient recalled after a month for check up showed periapical healing(fig-4d).
Procedure of placement of MTA
The tooth was isolated using a rubber dam and accessed. Magnification was used to facilitate all endodontic procedures on the tooth. The canal was gently debrided using large hand files and copious amounts of 5.25% sodium hypochlorite and saline irrigation. The working length was established and confirmed with radiographs. The canals were prepared to make parallel and smooth walls and dried. Mineral trioxide aggregate (M.T.A.) was introduced into the canal using a amalgam carrier and compacted with plugger to form an apical stop approximately 4-5mm thick. A radiograph was exposed to confirm adequate placement of M.T.A. The blunt end of a large paper point was moistened with water and left in the canal to promote setting of cement. A cotton pellet was placed in the chamber and the tooth restored with temporary cement. Patient was recalled after 3 days and accessed, the patient had remained asymptomatic and the tooth was isolated and accessed for complete setting of cement. A hand plugger was lightly tapped against the M.T.A plug to confirm a hardened set. The canal was obturated using custom made gutta-percha. The tooth was restored with glass ionomer cement and a recalled to check prognosis of tooth and further treatment
Discussion
A conventional approach to treat teeth with open apices is by use of calcium hydroxide and inducing apical barrier formation, during such treatment follow-up period the immature tooth is prone to fracture or re-Infection. Calcium hydroxide induced apexification requires 3 months to 24 months period15 Long term calcium hydroxide has also been reported to weaken the root structure16.MTA is gaining popularity for use as a apexification material with good physical and biological properties 7,8. In the present case1, there was no peri apical infection and patient insisted on treatment for discoloured tooth .Calcium hydroxide induced apexification was not possible as patient was not willing for the prolonged treatment procedure, hence MTA was considered as the best alternative. Case 2 had draining sinus and periapical infection hence calcium hydroxide was used to reduce infection and MTA was used as it has property to set in presence of moisture17.the presented cases showed that MTA can be used for root end restoration in cases with open apex and periapical infection. Follow up of cases showed periapical healing and formation of hard tissue in apical end of root of affected tooth. Al-Kahtani et al. 18 has recommended in his study placement of a 5-mm apical barrier of MTA in cases of apexification, as this allows excellent seal, and provides sufficient material thickness to prevent it from being displaced. Threma plasticized gutta-percha is usually recommended in these cases with thin walls but custom-made gutta-percha can also be used depending on the thickness of walls. In the present case both cases were obturated with custom made gutta-percha points as there was enough thickness of dentine. Placement of MTA has been considered in these cases as it is effective as an apical barrier and its application results in predictable apical closing, reduced treatment time and a reduced number of exposures to radiographs. Follow up after treatment of the case is of utmost importance to study the success of the treatment. In the present case 6 months of follow-up, the clinical and radiographic appearance of the teeth showed resolution of the periapical lesions and hard tissue formation at apex. The presented cases showed, placement of an apical barrier using MTA is an alternative to conventional long-term calcium hydroxide therapy.
References
1. LeeSJ,MonefM, Torabinajad.M. Sealing ability of a mineral tri oxide aggregate for repair of lateral root perforations.J Endo 1993;19:541-4
2. Schmitt D, Bogen G. Multifaceted use of ProRoot MTA root canal repair material. Pediatr Dent 2001; 23:326-30.
3. Sarkar NK, Caidedo R, Tirwik P, Moiseyeva R, Kawashima I.Physicochemical basis of the biologic properties of mineral trioxide aggregate. J Endod 2005; 31:97-100.
4. Camilleri J, Montesin FE, Brady K, Sweeney R, Curtis RV, Pitt Ford TR. The constitution of mineral trioxide aggregate.Dent Mater 2005; 21:297-303.
5. Dammaschke T, Gerth HUV, Zu¨ chner H, Scha¨ fer E.Chemical and physical surface and bulk material characterization of white ProRoot MTA and two Portland cements. Dent Mater 2005; 21:731-8.
6. David E. Witherspoon, BDSc, MS; Joel C. Small, DDS; Gary Z. Harris, DDS-Mineral trioxide aggregate pulpotomies A case series outcomes assessment JADA, Vol. 137 May 2006:610-618.
7. Enkel B, Dupas C, Armengol V, et al. Bioactive materials in endodontics. Expert Rev Med Devices 2008; 5:475-94.
8. Moretton TR, Brown CE Jr, Legan JJ, Kafrawy AH. Tissue reactions after subcutaneous and intraosseous implantation of mineral trioxide aggregate and ethoxybenzoic acid cement. J Biomed Mater Res 2000; 52:528-33.
9. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physical and chemical properties of a new root-end filling material. J Endod 1995; 21:349-53.
10. Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using mineral trioxide aggregate as a pulp-capping material.JADA 1996; 127:1491-4.
11. Torabinejad M, Chivian N. Clinical applications of mineral trioxideaggregate. J Endod 1999; 25(3):197-205.
12. Andelin WE, Shabahang S, Wright K, Torabinejad M. Identificationof hard tissue after experimental pulp capping using dentin sialoprotein (DSP) as a marker. J Endod 2003; 29:646-50.
13. Bakland LK. Management of traumatically injured pulps in immature teeth using MTA. J Calif Dent Assoc 2000; 28:855-8.
14. Schmitt D, Lee J, Bogen G. Multifaceted use of ProRoot MTA root canal repair material. Pediatr Dent 2001; 23:326-30.
15. Frank AL (1966) Therapy for the divergent pulpless tooth by continued apical formation.Journal of american Dental Association 72, 87-93.
16. Andreasen Jo,Farik B,Munksgaard EC(2002)Long term Calcium hydroxide as a root canal dressing may increase risk of root fracture. Dental Traumatology 18, 134-7.
17. Torabinajad.M, Watson.TF, Pitt Ford TR1993.Sealing ability of mineral tri oxide aggregate when used as a root end filling material.JOE-19,591-595.
18. Al-Kahtani A, Shostad S, Schifferle R, Bhambhani S (2005) In-vitro evaluation of microleakage of an orthograde apical plug of mineral trioxide aggregate in permanent teeth with simulated immature apices.J Endod 31,117-119.
19. Kratchman SI. Perforation repair and one-step apexification procedures. Dent Clin North Am 2004; 48:291-307.
20. Josette Camilleri- The chemical composition of Mineral trioxide aggregate-Journal of conservative dentistry-Oct- Dec- 2008, no11, issue 4;pg141-143. |