|
|
|
| Replantation Of An Avulsed Incisor: A Case Report |
Varun Jindal 1 , Deepti Jindal 2 , Aparna Palaker 3
1 Senior lecturer Department of Conservative dentistry & Endodontics - Bhojia Dental College & Hospital, Baddi, Distt. Solan
2 Senior Lecturer Department of Oral & Maxillofacial Pathology - B.R.S. Dental College & Hospital, Sultanpur, Panchkula
3 Professor, Department Of Conservative - Modern Dental College, Indore
|
| Address For Correspondence |
Dr. Varun Jindal M.D.S.
Department Of Conservative Dentistry & Endodontics
H.No:636,Sector-10, Panchkula, India, M:9876487103
Email id: varundeeptijindal@gmail.com |
| Abstract |
| Management of tooth avulsion in the permanent dentition often presents a challenge. Such injuries should be recognized and treated expeditiously because several studies support a more likely favorable prognosis with timely and appropriate initial management. This article describes the management of an avulsed maxillary permanent incisor that had been air-dried for about 2 hours. |
|
| Keywords |
| Avulsion, Replantation, Splinting, Clinical Management |
|
| Full Text |
INTRODUCTION
The term "dental avulsion" describes a clinical situation in which the tooth is completely displaced out of its socket following a traumatic impact1. Of all the dental injuries avulsion is by far the most serious because not only it severes the pulpal blood supply but it also expose the cells of the PDL to the external environment2.
It accounts for 0.5% to 16% of traumatic injuries in the permanent dentition. Avulsion of permanent teeth occurs most often in children 7 to 9 yrs. old, an age when the relatively resilient alveolar bone provides only minimal resistance to extrusive forces, and maxillary central incisors are the teeth most commonly affected3. Management of avulsion of the permanent dentition often presents a challenge. If the tooth is replanted promptly with a vital PDL, functional PDL healing can occur 4-10. The extraoral period significantly affects the outcome, influencing PDL vitality11. Clinical studies have shown that the prognosis is best for teeth replanted within 5 minutes after avulsion11-15.
Pulpal necrosis always occurs after an avulsion injury. While the necrotic pulp itself is of no consequence, the necrotic tissue is extremely susceptible to bacterial contamination. It revascularization does not occur or effective endodontic therapy is not carried out, the pulp space will inevitably become infected. The combination of bacteria in the root canal and cemental damage on the external surface of the root results in an external inflammatory resorption that can be very serious and lead to the rapid loss of tooth16. Nevertheless, if managed properly, avulsed teeth with a vital PDL can be replanted and will remain functional for some years17. This article describes the management of patient with an avulsed maxillary right central incisor.
CASE REPORT
A 30 year old male presented to the Department of Conservative Dentistry and Endodontics with dental traumatic injury after falling from a two wheeler. The accident resulted in avulsion and Ellis Class I fracture of maxillary right central incisor (Fig. 1) at the time of accident.
 | Fig 1. Preoperative View
 |
The maxillary right central incisor found at the site of accident was stored in milk and brought to the clinic the same morning at the time of presentation. Examination of the avulsed tooth revealed that the crown and root was intact (Fig.2).
 | Fig 2. Avulsed 11
|
Radiographs and clinical examination was done to rule out any other hard tissue injury. He had no other injuries and his medical history was uneventful.
The available treatment options were explained to the patient, and it was decided to replant the avulsed incisor as an intermediate treatment. Local anesthetic was administered and the blood clot removed from the socket. The tooth was then replanted into its socket. Splinting was done with a 0.018 inches stainless steel orthodontic wire bonded to the teeth with composite (Fig. 3).
 | Fig 3. Splinting Done From 13 To 23
|
Another radiograph was obtained to confirm proper positioning of the replanted incisor. A 5 day course of Amoxicillin was prescribed, and the patient was referred to the medical practitioner for an anti-tetanus booster.
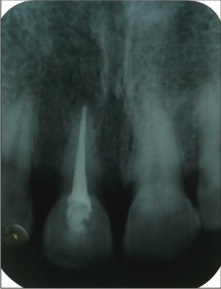
The patient was seen again at 1 week and at that time endodontic treatment was started. After 2 weeks endodontic treatment was completed (Fig.4)
 | Fig 4. Iopa After Root Canal Treatment
|
and splint was removed. Mobility of the teeth had reduced. Esthetic treatment for Ellis Class-I fracture was done with tooth colored resins.
DISCUSSION
Relative to other tooth injuries, avulsion is a more serious assault on the gingiva, the PDL and the pulp18. It has been reported that successful management of the avulsed tooth begins as soon as possible at the accident site. Extraoral time is important in determining the success of tooth re-plantation. Studies have shown that the prognosis of replanted teeth is best if re-plantation is carried out within 5 min. after avulsion19-21. In the case presented here extraoral time was less than 2 hrs, so it was anticipated that the chance of pulpal and PDL healing would be good.
Where the tooth cannot be replanted immediately the tooth should be stored in an appropriate medium such as normal saline, milk, saliva, hanks solution or water 22. In this case the tooth was kept in milk. It was reported that milk is shown to maintain vitality of PDL cells for 3 hrs being relatively bacteria-free with pH and osmolarity compatible with vital cells19.
Splinting is required routinely after replantation of avulsed teeth3. A splinting technique that allows physiologic movement of the tooth during healing and that is in place for a minimal time period results in a decreased incidence of ankylosis 23-26. Semi-rigid (physiologic fixation for 7-10 days is recommended23, 26. The splint should allow movement of the tooth should have no memory (so the tooth is not moved during healing) and should not impinge on the gingival and / or prevent maintenance of oral hygiene in the area. In this case splinting was done for a period of 2 weeks during which endodontic treatment was carried out.
Systemic antibiotics are often recommended after replantation, but their effectiveness in preventing root resorption is questionable27. To date the value of antibiotic therapy in replantation has been demonstrated only in the experimental setting28, 29. Andreasen and others11, in their prospective study, showed that systemic antibiotics had no effect on periodontal healing clinically.
Follow up evaluation was done at 1, 3 and 6 months after replantation. Radiographic evaluation showed no signs of external resorption (Fig.5, 6, 7, 8).
 | Fig 5. 1 Month Recall Radiograph
|
 | Fig 6. 3 Months Recall Radiograph
|
 | Fig 7. 6 Months Recall Radiograph
|
 | Fig 8. Postoperative View After 6 Months
|
CONCLUSION
Prevention and management of dental trauma should be recognized as an acute emergency. Prompt and early presentation for dental management in cases of avulsion is very important. Replantation can restore the patients esthetic appearance and occlusal function shortly after the injury, and the replanted teeth can remain functional for years.
REFERENCES:
1. Berman LH, Blanco L, Cohen Stephen. A Clinical Guide to Dental Traumatology: 2007 p. 100-126
2. Andersson L. Editorial: Tooth avulsion & Replantation. Dent Traumatol 2007;23:129
3. Andreasen JO, Andreasen FM. Textbook & Colour Atlas of traumatic injuries to the Teeth, 4th ed. Muksgaard; 2007 p444-488
4. Loe H, Waerhaugh J. Experimental replantation of teeth in dogs & monkeys. Arch Oral Biol 1961;3;176-84
5. Hammer JE III, Reed OM, Stanley HR. Reimplantation of teeth in the Baboon. J Am Dent Assoc 1970;81:662-70
6. Van Hassel HJ, Oswald RJ, Harrington GW. Reimplantation : the role of the periodontal ligament. J Endod 1980;6:506-8
7. Blomlof L, Lindskog S, Andersson L, Hedstrom KG, Hammerstrom L. Storage of experimentally avulsed teeth in milk prior to replantation. J Dent Res1983;62:912-6
8. Hammarstorm L, Blomlof L, Feiglin B, Andersson L, Lindskog S. Effect of calcium hydroxide treatment on periodontal repair & root resorption. Endod Dent Traumatol 1986;2:184-9
9. Wong KS, Sae-Lim V. The effect of intracanal ledermix on root resorption of delayed replanted monkey teeth. Dent Traumatol 2002;18:309-15
10. Andreasen JO. Periodontal healing after replantation & autotransplantation of incisors in monkeys. Int J Oral Surg 1981;10:54-61
11. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. 4. Factors related to periodontal ligament healing. Endod Dent Traumatol 1995; 11:76-89
12. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. 1. Diagnosis of healing complications. Endod Dent Traumatol 1995; 11(2):51-8.
13. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. 2. Factors related to pulpal healing. Endod Dent Traumatol 1995; 11(2):59-68
14. Andreasen JO, Borum MK, Andreasen FM. Replantation of 400 avulsed permanent incisors. 3. Factors related to root growth. Endod Dent Traumatol 1995; 11(2):69-75.
15. Kinirons MJ, Gregg TA, Welbury RR, Cole BO. Variations in the presenting and treatment features in reimplanted permanent incisors in children and their effect on the prevalence of root resorption. Br Dent J2000; 189(5):263-6.
16. Tronstad L. Root resorption etiology, terminology and clinical manifestations. Endod Dent Traumatol 1988;4: 241.
17. Duggal MS, Toumba KJ, Russell JL, Paterson SA. Replantation of avulsed permanent teeth with avital periodontal ligaments: case report. Endod Dent Traumatol 1994; 10(6):282-5.
18. Cho S, Cheng AC. Replantation of an avulsed incisor after prolonged dry storage: case report. J Can Dent Assoc 2002;68(5):297-300
19. Sanu OO, Utomi IL. Parental awareness of emergency management of avulsion of permanent teeth of children in Lagos, Nigeria. The Nig Postgrad Med Journ. 2005;12:115-120.
20. Marin PD. The avulsed tooth - the best implant. Ann R Australas Coll Dent Surgery. 2000;15:243-246.
21. Chan AWK, Wong TKS, Cheung GSP. Lay knowledge of physical education teachers about the emergency management of dental trauma in Hong Kong. Dent Traumatol. 2001;17:77-85
22. Trope M, Chivian N, Sigurdsson A, Vann WF., Jr . Traumatic injuries. In: Cohen S, Burns RC, editors. Pathways of the Pulp. 8. St. Louis: Mosby; 2002. pp. 636-637.
23. Andreasen JO, Andreasen FM. Textbook and Color Atlas of Traumatic Injuries to the Teeth, 3rd edn. Copenhagen and St. Louis, Munksgaard and CV Mosby, 1994.
24. Hammarstrom L, Lindskog S. General morphologic aspects of resorption of teeth and alveolar bone. Int Endod J 1985;18: 93-99.
25. Andreasen JO. Etiology and pathogenesis of traumatic dental injuries. Scand J Dent Res 1970; 78: 329-337.
26. Andersson L, Friskopp J, Blomlof L. Fiber-glass splinting of traumatized teeth. ASDC J Dent Child 1983;3: 21.
27. Barrett EJ, Kenny DJ. Avulsed permanent teeth: a review of the literature and treatment guidelines. Endod Dent Traumatol 1997; 13(4):153-63.
28. Hammarstorm L, Blomlof L, Feiglin B, Andersson L, Lindskog S. Replantation of teeth and antibiotic treatment. Endod Dent Traumatol 1986; 2(2):51-7.
29. Sae-Lim V, Wang CY, Choi GW, Trope M. The effect of systemic tetracycline on resorption of dried replanted dogs' teeth. Endod Dent Traumatol 1998; 14(3):127-32. |
|
|
|
|
|
|