|
|
|
| Invisalign- Emperor’s New Cloth |
N. Raghunath 1 , Shivalinga.B.M. 2 , Kanhu Charan Sahoo 3
1 Associate Professor, Dept. Of Orthodontics and Dentofacial Orthopaedics - J.S.S.Dental College and Hospital, Mysore, Karnataka
2 Professor and In-Charge of P.G. Studies Dept.Of Orthodontics and Dentofacial Orthopaedics - J.S.S. Dental College and Hospital, Mysore, Karnataka
3 Post Graduate Student, Dept. Of Orthodontics and Dentofacial Orthopaedics - J.S.S. Dental College and Hospital, Mysore, Karnataka
|
| Address For Correspondence |
Kanhu Charan Sahoo
Post Graduate Student
Dept. Of Orthodontics and DentofacialOrthopaedics
J.S.S. Dental College and Hospital, Mysore, Karnataka
Mob no: +91 9986673171
E-Mail: drkanhu@gmail.com |
| Abstract |
| The long-awaited paradigm shift in orthodontics has arrived with the introduction of the Invisalign system. Adult patients seeking orthodontic treatment are increasingly motivated by esthetic con¬siderations. The majority of these patients rejects wearing labial fixed appliances and are looking instead to more esthetic treatment options, including lingual orthodontics and Invisalign appliances. Since Align Technology introduced the Invisalign appliance in 1999 in an extensive public campaign, the appliance has gained tremendous attention from adult patients and dental professionals. The transparency of the Invisalign appliance enhances its esthetic appeal for those adult patients who are averse to wearing conventional labial fixed orthodontic appliances. Although guidelines about the types of malocclusions that this technique can treat exist, few clinical studies have assessed the effectiveness of the appliance and few recent studies have outlined some of the limitations associated with this technique that clinicians should recognize early before choosing treatment options. |
|
| Keywords |
| Esthetic Appliances, Stereo Lithography, Clincheck |
|
| Full Text |
Introduction:
Influence of appearance in personal and professional lives have led to a considerable interest among the adult population seeking orthodontic treatment in the last few years. Many esthetic appliance have come into market like ceramic brackets (and lingual appliance to cater the esthetic demands of adult population .One of the recent advancement being Clear Aligners. Clear plastic tooth moving appliance are excellent options for those adults who are reluctant to wear fixed appliance and whose chief complaint centers around mild to moderate alignment problems1.
History:
Zia Chishti and Kelsey Wirth were graduate students in Stanford University's MBA program. Zia Chishti had finished adult treatment with traditional braces, and wore a clear plastic retainer. He noticed that if he did not wear his retainer for a few days, his teeth shifted slightly-but the plastic retainer soon moved his teeth back the desired position.
Together they started Align Technologies in April 1997 and with the help of a handful of forward thinking orthodontists, they applied 3-D computer imaging graphics and created the Invisalign method. This appliance was the first orthodontic treatment method to be based solely on three-dimensional (3D) digital technology. Align Technologies received FDA clearance to market Invisalign in August 1998, and began commercial operations in July 1999.
Over view (Fig-2):
PVS impression, waxbite, radiographs, photos.
CT scan of the impression to produce virtual model.
Treat II software used to simulate the teeth movement.
Clincheck allows Orthodontist to reviews, modify, and approve the treatment plan. Stereo lithography treatment cast build precise models of teeth at each stage Individualized, custom-created clear aligners are made from these models.
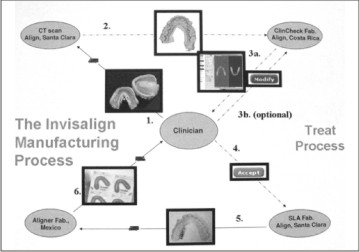 | Fig-2- Over View Invisalign Technique
 |
Diagnosis and Treatment Planning (Selection criteria) 2:
Fully erupted permanent teeth,
Growth has minimal or no effect on treatment (i.e., late adoescents and adults). ©Mild spacing (1-3 mm), moderate spacing (4-6 mm),
Mild crowding (1-3 mm), moderate crowding (4-6 mm),
Narrow arches that are dental in origin (4-6 mm),
Treated cases with relapse
Orthodontic movements which can be produced effectively:4,5,9 &10
Space closure
Tooth movement following Interproximal reduction
Dental (not skeletal) expansion,
Flaring
Distalization
Space closure following the extraction of a lower incisor
Certain malocclusion more difficult to treat3, 5:
Crowding and spacing over 5mm.
Skeletal antero-posterior discrepancies
Centric relation and centric occlusion discrepancies.
Severely rotated teeth (more than 20 degrees).
Open bites (anterior and posterior).
Extrusion of teeth
Severely tipped teeth (more than 45 degrees).
Teeth with short clinical crowns.
Arches with multiple missing teeth.
Closure of bicuspid extraction spaces
Steps in treatment:
Complete an Invisalign System™ diagnosis treatment planning form specifying movements one wishes to make over the course of treatment as well as the desired final occlusion. Submit copies of all diagnostic records and treatment plans for review and approval by Align Technology orthodontists.
Polyvinyl Siloxane (PVS) Impressions:
Polyvinyl siloxane is the impression material of choice because it yields highly accurate impressions that remain stable for as long as three weeks and allows for multiple pours.
The two-step recommended protocol:
Loose-fitting custom tray from a heavy body impression material.
Actual impression itself, made from a light body material that produces a highly accurate negative reproduction of the hard and soft tissue anatomy of the dental arch.
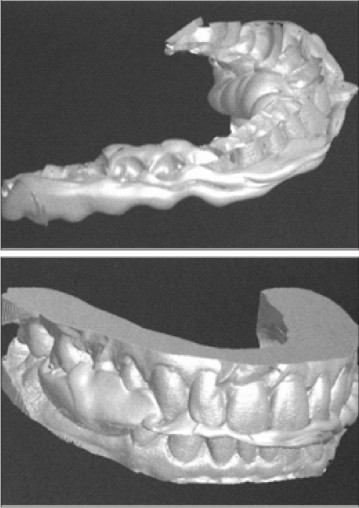
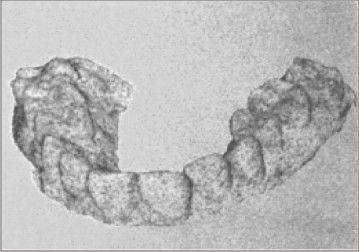
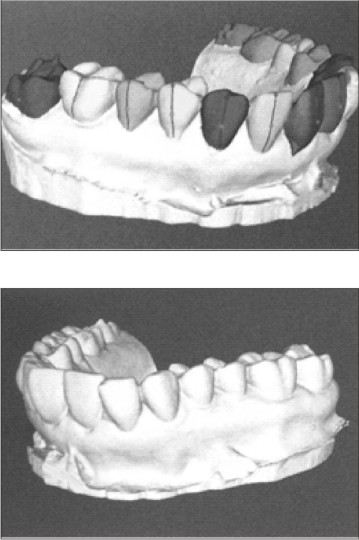
The Digitization Process:
The patient's polyvinyl siloxane (PVS) impressions and bite registration must first be converted into dimensionally accurate 3- dimensional electronic study models by means of a Computer Aided Tomography (CAT) scan (Fig-1 A-1C).
 | Fig-1 A to 1 C- Bite Registration Converted To 3-D Models.
|
To create a virtual dental model directly from the impression with CT scanning, the impression is mounted on a platform that rotates in front of an amorphous silicon x-ray sensor .Hundreds of digital radiograph of the impression are captured as it rotation 360°. These radiographs are converted to images called sinograms, which represent the data from a horizontal line of the detector as the part rotates.
3 D Virtual models:
These slices are stacked electronically and inverted, and the resulting surface is smoothed to yield a raw electronic study model.
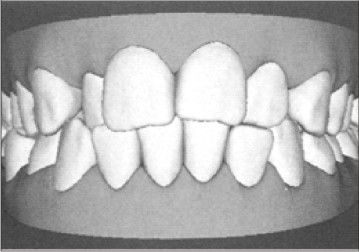
The virtual set up:
Once the virtual models are produced they are then sent electronically to Align's facility in Costa Rica where the raw electronic models are "detailed" by using software that simulates standard dental lab procedures, such as bubble removal, void filling, and gingival-line definition.
Then the 3D image is accessed by technician who transforms the raw data into a plan for the manufacture of custom aligners (Fig- 3A-3C).
The process is comprised of 3 phases
 | Fig-3- Virtual Model Set Up
|
Cutting Process
Creating the final setup
Staging process
Align Technology uses TREAT® software which is sophisticated 3D graphics program that gives the operator great control of tooth position as well as rate of tooth movement.
Cutting Process:
Virtual tools in the form of planar and curved cutters that are part of the Treat software are used to isolate data for each tooth within the arch into separate geometric units.
Creating the Final Setup:
Each crown is painted to distinguish between the tooth anatomy and gingival tissue. Landmarks such as the facial axis of the clinical crown of each tooth are identified. Now the separated teeth can be moved as individual units into arch form. The technician moves the specific teeth into alignment creating a final setup which precisely matches the doctor’s prescription.
Staging process:
The next step in the process is to determine the number of intermediate stages (and thus the number of aligners) between the original malocclusion and the final treatment result.
The two factors
Path of tooth movement
Velocity at which the teeth are to be moved. The maximum velocity of tooth movement currently is 0.20-0.25 mm per tooth per stage. The greater the distance that the teeth need to be moved or rotated and the more complicated the movement path, the greater the number of aligners needed to treat the patient The number of aligners varies from ten or less for relatively simple problems to fifty aligners or more in complicated malocclusions.
ClinCheck software:
After the forecast model and treatment sequence have been generated, this information is sent over the Internet to the orthodontist, who reviews the forecast model and sequence by way of the ClinCheck® soft¬ware program.
The ClinCheck set-up can be used:
For Diagnosis and treatment planning evaluate the need for IPR, expansion, extraction, distalization, or proclination.
For verifying that technician has performed modifications.
As a consultation device to show treatment limits to patient.
For verifying if aligner is tracking.
Clin Advisor:
On October 17, 2006, Align also announced the rollout of ClinAdvisor(TM), a new suite of software tools designed to make Invisalign case selection, submission and review processes more efficient for doctors.
ClinAdvisor simplifies case selection by helping doctors identify the skills necessary for a specific case. A complexity rating system categorizes treatment plans as "Easy," "Moderate" or "Advanced" and lists expected treatment characteristics and potentially challenging movements for each option.
Doctors have the option of choosing from four separate treatment goals for more efficient treatment planning:
Pre-Restorative: helps prepare teeth for restorative procedures
Esthetic: aligns the upper and lower anterior teeth
Anterior Function Improvement improves the canine relationship in addition to esthetic alignment
Optimal Setup: addresses all aspects of malocclusion.
Stereo lithography (Fig-4):
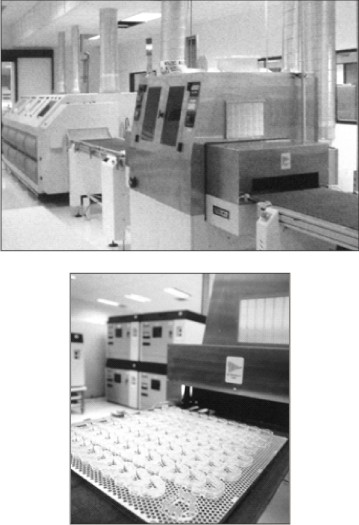 | Fig-4-Steriolithographic processing unit
|
An orthodontic product like Invisalign requires from 6 to 40 sequential appliances per arch; manual fabrication of this many appliances would be prohibitively expensive, and it would be difficult to maintain the required accuracy.
Instead, Align Technology uses stereo lithography technology to create its reference models Stereo lithography (SLA) is a rapid prototyping process by which a product is created using a Ultra-violet (UV) curable liquid resin polymer and advanced laser technology. These SLA resin models are loaded into an automated aligner-forming system that heats, forms, and laser-marks sheet plastic over each model.
These parts are transported on a conveyor belt to a robotic arm that loads each part into an automated cutting machine for trimming where they are trimmed to within ½ mm of gingival margin for patient's optimal comfort and minimal visibility. Automation enables aligner trimming to be completed in less than 30 seconds (Fig-5).
Once trimmed, the part is ejected, and the aligner is separated, laser-etched with the patient's initials, case number, aligner number, and arch (upper or lower) then polished, disinfected, and packaged for shipment to the customer.
 | Fig-5- Trimming of Aligner
|
Aligner Material
Invisalign appliances are composed of polyurethane with added methylene diphenyl diisocyanate and 1, 6 hexanediol. Polyurethane, the basic constituent polymeric component of Invisalign aligners, is not an inert material and is affected by heat, moisture, and prolonged contact with enzymes. At present Align Technology is using Exceed-30 (EX30) as aligner material as it is more flexible (easier to use with attachments), moreover it rarely breaks and remains clear. Exceed-40 (EX40) is used as retainers.
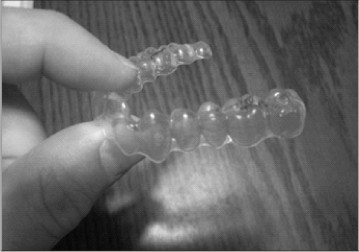 | Fig-6- Aligner Material
|
Attachments (Fig-7A & B):
Align Technology defines attachments as three dimensional shapes added to tooth geometry to enhance the interaction between an Aligner and the teeth.
These are represented by the red shapes seen on some teeth in ClinCheck® that translate into an equivalent geometry built into the aligner.
 | Fig-7- Aligner Attachment
|
Attachment Protocol:
Align Technology will automatically place attachments wherever required. One may request attachments for any of tooth movements by specifying in the special instructions box of the treatment form or in the comments box in ClinCheck.
Orthodontic Treatment with Invisalign:
The initial treatment visit involves inserting the first appliance of the series and carefully checking to be sure the appliances are fully seated.
Some patients require attachments to their teeth to facilitate certain movements such as extrusion, extraction space closure or rotation of lower premolars.
Aligners typically are worn for 24 hours daily; the patient is advised to remove them only while eating, drinking, brushing and flossing.
Aligner’s are commonly worn for 7 to 14 days, with progress being patient and movement specific.
Protocol for changing aligners:
Recently Align developed a more rigid standard for magnitude of tooth movement which now requires two weeks for each Aligner (24 hours daily).
May be more than two weeks per aligner in extraction cases with bodily movement, for patients who wear Aligners less than 22 hrs/day, or if problems occur with Aligner seating completely.
Patients should keep die last 3 to 4 Aligners in order to go back to a stage that fits if seating problems occur If the patient does not wear an aligner for more than 2-3 weeks, nrv; PVS impressions and rescanning may be necessary.
If patient loses an Aligner, they should try the next aligner (wear for one month) or use the previous aligner.
Aligner fit:
The aligner must fully "cup" the tooth crown at all times to prevent the occurrence of aligner length/arch length discrepancy .Thus, it should be understood that poor vertical fit of the aligner promotes mesio-distal problems. The aligner can fully seated with the help of Chewies made of polyurethane foam.
Retention:
Usually, the final appliance or a thicker version - 0.04 inch i.e. (Exceed-40 (EX40) of it, is worn full-time for 6 months.
Aligner cleaning:
Brush with toothbrush (powered better)
Soak for 5 minutes with-new-Align dissolving tablets or 3-4 drops of Clorox (both sodium hypochlorite) in lukewarm water.
Advantages8:
Esthetic-rarely noticed even at close distance- attracts additional patients.
Removable - unlike fixed appliance, one can eat and drink what one wants during treatment
Comfortable - no metal brackets or wires to cause mouth irritation
Better oral hygiene than fixed
Teeth can be bleached with the appliance at the beginning and during treatment
Shorter appointments
Decreased doctor & auxiliary time
Decreased allergic response (no metal or latex) - aligners are made from polyvinyl material
Retention facilitated (does not require a new patient experience)
Ideal for retreatment
Decreased occlusal abrasion from para-functional habits during treatment
Disarticulation of the teeth may be advantageous for patients with TMJ problems
Technically much easier than lingual appliances
Ability to present case to patient with final result prior to treatment.
Limitation11, 12:
Primary among them is compliance. Because the aligners are removable, the orthodontist must rely on the patient's motivation and dependability to achieve the desired results. The removability of Invisalign is an advantage to the patient but not to the clinician. So, its biggest advantage becomes its biggest disadvantage.
All permanent teeth should be fully erupted for treatment using this appliance, as it is difficult to achieve retention of the appliance on short clinical crowns.
There is currently no capability to incorporate basal orthopedic change with this appliance system, thus restricting it to malocclusions requiring purely dental movement.
Due to the fact that the surface anatomy of the teeth cannot undergo change during treatment as it will affect-the fit of aligners, major restorative work should be performed fore the commencement of treatment.
Lack of operator control - Unlike fixed or other types of removable appliances, the treatment plan cannot be changed once the appliance series has begun.
Inability to integrate hard and soft tissues of the head into the computer treatment. Thus, the clinician has no direct indication of where teeth are in relation to basal bone or in relation to the lips or other soft tissues of the head.
Conclusion:
With Invisalign the major advantage is the esthetic, hygienic, low discomfort and removable nature of the appliance. There are currently limitations to this appliance in terms of case selection, increased cost, experience required for computer treatment planning, difficulty obtaining certain tooth movements, and the lack of potential in cases involving mixed dentition or impacted teeth. One needs to understand that Invisalign is only an appliance, and the technique for working with it is continually being developed and honed. Refinement, adjustment at each appointment, and rebooting are all part of the technique, and all depend on the orthodontist's skill-just as with a patient in any fixed appliance.
References:
1. Introducing Invisalign. The invisible way to straighten your teeth without braces. Available at:http://www.invisalign.com/generalapp/gb/en/index.html. Accessed May, 2006.
2. Joffe L. Invisalign: early experiences. J Orthod 2003; 30(4):348–52.6. Lindauer SJ, Shoff RC. Comparison of Essix and Hawley retainers. J Clin Orthod 1998; 32(2):95–7.7.
3. Bollen AM, Huang G, King G, Hujoel P, Ma T. Activation time and material stiffness of sequential removable orthodontic appliance. Part 1: Ability to complete treatment. Am J Orthod Dentofacial Orthop 2003; 124(5):496–501.8.
4. Miller RJ, Duong TT, Derackhshan M. Lower incisor extraction treatment with the Invisalign system. J Clin Orthod 2002; 36(2):95–102.9.
5. Womack WR, Ahn JH, Ammari Z, Castillo A. A new approach to correction of crowding. Am J Orthod Dentofacial Orthop 2002; 122(3):310–6.10.
6. Clements KM, Bollen AM, Huang G, King G, Hujoel P, Ma T. Activation time and material stiffness of sequential removable orthodontic appli¬ance. Part 2: Dental improvements. Am J Orthod Dentofacial Orthop 2003; 124(5):502–8.11.
7. Kamatovic M. A retrospective evaluation of the effectiveness of the Invisalign appliance using the PAR and irregularity indices [dissertation]. Toronto (Ont.): University of Toronto; 2004.
8. Djeu G, Shelton S, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop 2005; 128(3):292–8.13.
9. Vlaskalic V, Boyd R. Orthodontic treatment of a mildly crowded malocclu¬sion using Invisalign system. Aust Orthod J 2002; 17(1):41–6.14.
10. Boyd RL, Miller RJ, Vlaskalic V. The Invisalign system in adult orthodontics: mild crowding and space closure cases. J Clin Orthod 2000; 34(4):203–12.
11. Boyd RL. Surgical-orthodontic treatment of two skeletal Class III patients with Invisalign and fixed appliances. J Clin Orthod 2005; 39(4):245–58.5.
12.Xiem Phan, BSc, DDS; Paul H. Ling, DDS, MDS Ortho. Clinical Limitations of Invisalign. JCDA 2007 April; 73(3): 263-66.
|
|
|
|
|
|
|