INTRODUCTION
Phonetics is the study of vocal sounds. Communication between the individuals is the basis for civilized growth of the community and speech dominates human communication. The ability to produce, manipulate and articulate with sounds is called speech. Variations in the same are manifested as slight differences in the pitch, tone and articulation of sounds that we make during the course of a normal conversation. Phonetics (from the Greek (phonê) "sound" or "voice") is the study of the physical sounds of human speech. It is concerned with the physical properties of speech sounds (phonemes), and the processes of their physiological production, auditory reception, and neurophysiological perception.
Phonetics was studied as early as 2,500 years ago in ancient India, with Panini's account of the place and manner of articulation of consonants in his 5th century BC treatise on Sanskrit. The major Indian alphabets today order their consonants according to Panini's classification. Speech is a very sophisticated autonomous and unconscious activity.
The loss of teeth and supporting structures alters the main oral cavity and produces a significant effect on the speech pattern. A scientific approach to the phonetic factor in denture construction often places the burden on the tongue to adapt, so as to compensate speech changes. If dentures are to contribute effectively to the functions of speech, dentists should utilize studies in the speech science field to implement their clinical knowledge of the phonetic factor in denture construction.1
Speech And Its Components:
All speech sounds are produced by controlling the airstreams that is initiated in the lungs and passes through the larynx and vocal cords. Speech sound requires more air than quiet exhalation; consequently, subtle adjustments in air flow contribute to variations of pitch and intensity of the voice. The structural controls for speech sounds are the various articulations or valves made in the pharynx and the oral and nasal cavities. Each sound is affected by the length, diameter and elasticity of vocal tract and by the locations of constrictions along its length.
Kantner and West divided speech into 5 components:-
1. Respiration
2. Phonation
3. Resonation
4. Articulation
5. Neural integration
Chierici and Lawson added a sixth component i.e. audition or the ability to hear sounds, to this list.
6. Audition
Sounds
Sounds are produced by passing a stream of air from the lungs through one or more resonators.
Resonators are
Pharyngeal cavity
Oral cavity
Labial cavity
Nasal cavity
Sounds can be categorized as consonants and vowels, voice and nasals.
Consonants and Vowels
The distinction between consonants and vowels is made in the following manner.
If the air, once out of the glottis, is allowed to pass freely through the resonators, the sound is a – vowel.
If the air, once out of the glottis, is obstructed, partially or totally, in one or more places, the sound is a – consonant
Before proceeding, it should be noted that the line between vowels and consonants cannot be clearly drawn; a continuum exists between the two extremes. There are also, intermediate instances, such as the semi-vowels and the (frictionless) spirants.
Voice
A sound is described as voiceless when the vocal cords do not vibrate during its articulation. If the vocal cords do vibrate, the sound is called voiced. The vocal cords are folds of muscle located at the level of the glottis (in fact, the glottis is nothing other than the space between the vocal cords). The vocal cords vibrate when they are closed to obstruct the airflow through the glottis. They vibrate under the pressure of the air being forced through them by the lungs. The voiced/voiceless opposition is mainly useful for the classification of consonants
Nasal
The top of the pharynx is like a crossroad. The airstream can exit the pharynx either of two ways, depending on the position of the soft - palate:
If the soft palate is lowered, a portion of the air will pass through the nasal cavity (the remainder finding its way through the oral cavity); if the soft palate is raised, access to the nasal cavity is cut off, and the air can only pass through the oral cavity. The sounds produced via the first method are called nasal; those produced the other way oral.
Plosives, Fricatives, Laterals And Vibrants
Plosives
Plosives, also known as Stops or Occlusives, are formed by completely blocking off the air flow. This blockage is only temporary: one way to think of it is that the air builds up and eventually explodes open the air passage (hence the name plosive). Sounds like P, B, M, T, D.
Fricatives
The name fricative comes from "friction." When you produce a fricative, instead of blocking off the flow of air for a short time (like you did with the plosives) the air is always let through. However, it is let through a very narrow space. The friction of the air moving through this narrow space is what creates the sound.
Fricatives are described as hissers and husher (Fig. 1). The realization of a hisser requires a high degree of tension in the tongue; a groove is formed along the whole length of the tongue, in particular at the place of articulation where the air passes through a little round opening. The hushers are produced similarly, but with a shallower groove in the tongue, and a little opening more oval than round. The lips are often rounded or projected outwards during the realization of a husher.
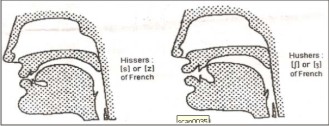 | Fig. 1 - Hissers (left) and Hushers (right)
 |
Laterals
They are "L"-like consonants pronounced with an occlusion made somewhere along the axis of the tongue, while air from the lungs escapes at one side or both sides of the tongue. Most commonly the tip of the tongue makes contact with the upper teeth or the upper gum (the alveolar ridge) just behind the teeth.
Laterals are generally considered to be a special case, they could be grouped among the fricatives and spirants. They are called laterals since during their production, the back of the tongue makes contact with the hard palate while the front of the tongue sinks down, channeling the air laterally around the tongue, down the side (or sometimes both sides) of the mouth. (On the other hand, for non-lateral articulations, the back of the tongue rests against the top molars, and the air flows over the tongue down the center of the mouth)(Fig. 2).
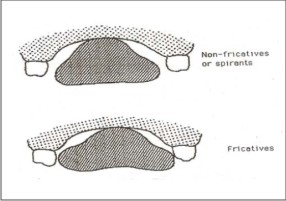 | Fig. 2 - Position of tongue in lateral fricatives and spirants
|
There are two distinct types of lateral:
Lateral fricatives, where the articulation, requiring a great deal of muscular tension, resembles that of the fricatives (except for the position of the tongue); Non-fricative lateral often called liquids, whose articulation is very close to the spirants.
The location of the lateral channel through which the air flows is unimportant: whether it is on the left, the right, or both sides of the mouth. The nature of the sound produced is unchanged.
Lateral Fricatives
Voiceless dental or alveolar lateral fricative
For the dental, the tongue tip makes contact with the inside of the upper teeth; for the alveolar, the tongue tip rests on the alveolar ridge. The tongue is strongly flexed and the air is forced through a narrow oval cavity, producing a hushing sound.
Voiced dental or alveolar lateral fricative
Same as above, but with vibration of the vocal cords.
Non-Fricative Lateral
Non-fricative laterals or liquids, which are rather spirant-like in character. No distinction is made here between voiceless and voiced variants (it is very rare to for a language to distinguish laterals according to voice).
Dental or alveolar non-fricative lateral
For the dental, the tongue tip makes contact with the inside of the upper teeth; for the alveolar,
the tongue tip rests on the alveolar ridge. The air flows over the sides of the tongue.
Retroflex non-fricative lateral
The tip of the tongue curves up and back and its underside makes contact with the roof of the mouth. The sides of the tongue are lowered to allow the passage of air.
Palatal Non-Fricative Lateral
The front part of the tongue is pressed against the hard palate. The tongue is arched to allow
the passage of air.
Vibrants
These consonants involve one or more tapping or flapping vibrations of the speech organs under pressure from the airstream. Part of the tongue makes contact with the palate, most commonly at the alveolar ridge, the soft palate, or the uvula. Vibrants are generally voiced.
There are two distinct classes of vibrant:
Taps – with only one vibration
Trills – with multiple vibrations
Role of Speech In Prosthodontics
The restoration of form and function of missing teeth and oral structures not only denotes esthetics and mastication, but also phonetics. Phonetics, if applied correctly can aid in the fabrication of a physiologically as well as functionally sound prosthesis.
In Complete Denture
1. In the orientation of anterior teeth: -
The following sounds can be used as a guide to the placement of teeth and adjust the thickness and extension of denture flanges in complete denture construction 1,2 .
A). Labial sounds - b, p, m. produced -at the lips (anterior posterior position of teeth)
The sounds ‘b’, ‘p’ and ‘m’ are made at the lips. In ‘b’ and ‘p’ air pressure is build up behind the lip and released with or without a voice sound. Insufficient support of the lips by the teeth and the denture base can cause these sounds to be defective. Therefore, antero posterior position of the anterior teeth and the thickness of the labial flanges of the denture can affect ‘b’ and ‘p’ sounds.
Likewise, incorrect vertical dimension of occlusion (VDO), teeth positioning hindering proper lip closure, cleft lip or incompetent upper lip might influence these sounds.
B). Labio-Dental sounds – f, v (vertical position of teeth)
Made between the upper incisors and posterior or middle 1/3 (Labiolingual) of the lower lip.
F, v & ph are the labiodental sounds between the upper incisors and the labiolingual centre to
the posterior one third of the lower lip.
Affected by the supero-inferior positioning of the upper incisors.
If incisors too high up (or too short) - v will sound like f.
If too low (Long)-
f will sound like v.
C).Dental and Alveolar Sounds (labiolingual position of teeth)
Dental- th. Made with the tip of the tongue extending between upper and lower anterior teeth. The tongue is actually closer to the alveolus
If 1/8th inch of tongue not visible - Anteriors placed too forward. (Except in Class II)or excess vertical overlap.
If more than 1/4th inch
tongue visible - Teeth positioned too lingual.
Alveolar - t, d, n, s and z. Formed by a valve formed by tip of tongue with the anterior – most part of the palate (alveolus) or lingual surface of anteriors.
If teeth too lingual - t will sound like d
If teeth too forward - d will sound like t
(Same effect for the thickness of denture base at rugae).
D). Sibilant –s, z, zh, ch, j sounds
Affected by the relationship of the anterior teeth to each other. Anterior teeth should approach end to end, but should not touch while these sounds are made. Can be used to check the total length (vertical dimension), vertical and horizontal overlap.
The ‘S’ sound is considered both a dental and alveolar sound because it can be produced equally well with two different tongue positions. Most people make ‘S’ with the tip of the tongue against the alveolus in the area of the rugae, with a small space for the air to escape, the size and shape of this space decides the quality of the sound (Fig. 3).
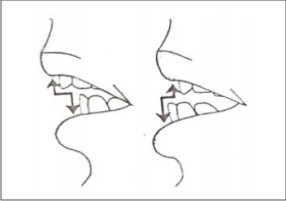 | Fig. 3 - Incorrect (Excessive and deficient) horizontal overlap of the anteriors during production of sibilants
|
When patients pronounce s, z and c, the mandible comes forward and the tip of the tongue is in contact with the most anterior part of the hard palate. The lateral borders of the tongue are in light contact with the lingual surface of the posterior teeth. When channel formed between the tongue and the palate is narrow, air is forced through with a hissing sound resulting in the production of these sibilants.
Lisping And Whistling
If the anterior portion of this channel is round and oval, i.e. too large, the hissing becomes a whistle. If the entire channel is too broad, ‘S’ sounds like ‘sh’, i.e. lisping occurs 3.
If the air channel is blocked completely with the tip of the tongue pressed completely against the rugae, the air is forced to escape on both sides of the tongue and ‘s’ sounds like ‘sh’ ((Fig. 4).
The production of ch, s and j sounds brings the anterior teeth close together, and when correctly placed, the lower incisors should move forward to a position directly under and almost touching the upper central incisors. If the distance is too large, the vertical dimension of occlusion established may be too small, and if the anterior teeth touch when these sounds are made, the vertical dimension is probably too great. This space that is visible between the upper and lower anteriors when the sibilants are being pronounced is called "Silverman's closest speaking space".
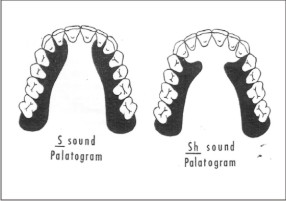 | Fig. 4 - Palatogram during production of 's' and 'sh' sounds
|
E).Palatal and Velar sounds.
Palatal - Year, She, Vision are not influenced much by the teeth.
Velar - K, G, ng etc. Not affected by dentures.
2. Establishing incisal guidance
'F' or “V" & 'S' Speaking Anterior Tooth Relation...
An another method devised by Pound & Murrel, for establishing the incisive guidance by arranging the anterior teeth in the occlusal rims -before recording the vertical dimension of occlusion. The position of the artificial maxillary anterior teeth is determined by the position of the maxillae when the patient says words beginning with T or 'v'; the mandibular anterior teeth by the position of the mandible when the patient says words beginning with ‘s’ (Fig.5). The mandibular cast with the 'speaking wax' is used, which is soft bees wax supported by hard modeling wax, and the patient is asked to pronounce different words with the requisite sounds and the recording made.
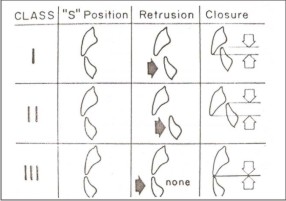 | Fig. 5 - Relation of the anterior teeth at the's' position for three classified jaw relations for retrusion and closure.
|
3. Establishing vertical dimension
During recording of the patient's vertical dimension at rest, the mandible is brought to the physiological rest position using numerous methods, and phonetics also guides in the same. Initiating a conversation with the patient aids in inadvertently relaxing the patient and removing the self-consciousness factor which often prevents the patient from being relaxed and bringing the mandible to rest position4.
Meyer M Silverman (1953) 5 concluded that the speaking method of measuring vertical dimension is a physiologic phonetic method which measures vertical dimension by means of the closing and speaking space. Distance between centric occlusion line and closest speaking line is called the closest speaking space. Closest speaking space is measurement for vertical dimension. This space varies in different individual and ranges from 0-10 mm (Fig. 6)
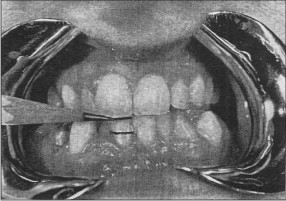 | Fig. 6 - Top line closest speaking line and bottom line showing occlusal line
|
PALATOGRAMS IN COMPLETE DENTURES
Palatograms are the area of tongue contact for a given sound displayed on an artificial palate through a medium of non scented talcum powder.
Pre-Requisites of Making a Palatogram
1. The artificial palate must be accurately adapted and refined so that it can be worn comfortably without an adhesive until speech is normal and natural. The subject who does not accommodate or who gags after a 15 minutes practice speaking period should not be used, because palatograms of faulty speech would be of dubious value and gagging makes palatography impossible.
2. The subject should be trained to pronounce the sound distinctly, then to open his mouth with the tongue flat (out of contact with the palate) and not to attempt to swallow until after the palate is removed. Several trials should precede the making of the palatogram to ensure that the patient can pronounce the sound distinctly and immediately open his mouth without a gain contacting the palate with the tongue.
3. The tracing medium should not be distasteful in flavors or appearance and should be of a consistency that will permit ease of application and removes from the artificial palate. The color of the medium should contrast with the palate sufficiently to display readily the area of tongue contact.
4. The palate must be dried thoroughly before dusting with talc, and care must be taken in inserting and removing the dusted palate to avoid finger contact, which would smudge the tracing. In pronouncing the phoneme, the moist tongue removes the talc from the contact area, leaving a clear tracing.
Allen (1958)6 advocates making the palatal portion as thin as is practical. Overall dentures range from 0.5 mm to 10 mm in thickness.
In Removable And Fixed Partial Denture
Many of the factors affecting the placement of teeth in complete dentures also act pertaining to partial prosthodontics. But clinical evidence often reveals that there is very little or no loss of the ability to phonate correctly7,8. This is due to the fact that there is only a partial loss of teeth and these patients are younger and hence show better neuromuscular coordination than complete denture patients. The patients show enough dexterity to adapt to individual situations and the defects in phonation are often not discernible.
In fixed prosthodontics, in anterior restorations, the pontic and connector design is very important. If there is poor adaptation of the pontic to the ridge, either due to faulty design or due to residual ridge resorption, there is air escape through the tissue surface of the pontic while speaking, especially during the production of sibilants causing faulty phonation.
In Maxillofacial Prosthodontics
Surgical, Congenital or Developmental defects in the peripheral organs of phonation and the associated maxillofacial complex severely compromise the ability of the subject to speak properly 9. The aim of the Prosthodontist should be not only to restore form, but also to restore function in terms of mastication and optimum phonetics. Often, a speech pathologist works in conjunction, to train the patient to adapt and adjust to the available compromised maxillofacial situation and function.
Tachimura T, Nohara K, Hara H, Wada T (1999)10 concluded that the severity of velopharyngeal incompetence might be related in part to change in levator activity in association with oral air pressure.
Of the six components of speech, resonance and articulation are the most readily influenced my maxillo-facial prosthodontics. These two components are intimately related and difficult to separate into distinct entities for purposes of clinical evaluation. Patients with acquired defects or congenital malformations of the soft palate may exhibit excessive nasal resonance, because without surgical and/or prosthodontic intervention, they are unable to control and divert sufficient airflow into the oral cavity. Whereas velo-pharyngeal closure remains the major determinant of resonance balance, other factors such as tongue position and structural resistance within the nasal cavity, influence the perceived oral-nasal resonance balance.
CONCLUSION
Basic laryngeal vibrations modified by fixed and mobile articulators produce speech. The tongue is a major articulator during the production of all phonemes, with the exception of bilabial and labio-dental sounds. It modifies the shape of the oral cavity, thus changing the resonance characteristics required for the production of various vowels, and completely or partially occludes the vocal tract producing different consonant sounds. Another factor influencing the production of sounds is the integrity and neuro-muscular health of the oral and peri-oral structures like the lips, cheeks, teeth, alveolus, palate ( hard & soft), larynx and the respiratory system. Thus, speech is a collective response to the action of all the above mentioned supplementary factors.
References
1. Zarb GA, Bolender CL, Eckert SE, Jacob RF, Fenton AH, Mericske-Stern R. Prosthodontic Treatment for Edentulous Patients. 12th ed., Mosby; 2004. p. 379-87.
2.Sharry John J. Complete Denture Prosthodontics. 3rd ed., McGraw-Hill Book Company;1974. p. 130-48.
3. Silverman M. Meyer. The whistle and swish sound in denture patients. J Prosthet Dent 1967; 17: 144-8.
4. Silverman M. Meyer. The speaking method in measuring vertical dimension. J Prosthet Dent 1953; 3: 193-9.
5. Silverman M. Meyer. Vertical dimension must not be increased. J Prosthet Dent 1952; 3: 193-9.
6. Allen L.R. Improved phonetics in denture construction. J Prosthet Dent 1958; 8:753-63.
7. Carr Alan B, McGivney P, Brown David T. McCracken’s Removable Partial Prosthodontics. 11th ed. Mosby; 2005. p. 397-426.
8. McGivney GP, Castleberry DJ. McCracken’s Removable Partial Prosthodontics. 8th ed. CBS Publishers; 1989. p. 437.
9. Beumer J, Curtis TA, Marunick MT. Maxillofacial Rehabilitation: Prosthodontic & Surgical Considerations. St. Louis: Elsevier; 1996. p. 285-329.
10 Tachimura T, Nohara K, Hara H, Wada T. Effect of placement of a speech appliance on levator veli palatini muscle activity during blowing. Cleft Palate Craniofac J 1999; 36:224-32. |