INTRODUCTION
The search for an ideal and universally acceptable system to restore pulpless teeth is still a goal of dental materials research.
Compared to teeth with healthy pulp, root filled teeth are considered more susceptible to fracture as they possess reduced dentinal elasticity, lower water content, deeper cavities and substantial loss of dentin.1. Controversy exists as to whether endodontic procedure are the primary cause for the loss of strength for a tooth. It was concluded that endodontic procedures had only a small effect on tooth strength. Rather, it was the advancing preparation that caused reduction in relative stiffness of tooth.2
The ability to predictably restore an endodontically treated tooth to its original strength and the fracture resistance without placement of a full coverage restoration could
provide potential periodontal and economic benefits to patients. Several researchers have reported that bonded composite restorations will better strengthen a tooth compared with Amalgam. As a result of recent developments in composite resin technology, new restorative materials with improved mechanical and physical properties such as hybrid and packable composites have been introduced in the market.4
The new class of resin composites, high viscosity, packable composites whose handling has been modified to mimic the condensability of the amalgam. Ormocers, organically modified ceramics having filler size 0.8 ƒÝm and 82% by weight that consist of organic – inorganic copolymer and inorganic silanated filler particles. This material is stiffer, having increased strength due to ceramic fillers and less sticky than traditional composites.5 Hybrid composite ClearfilTM AP-X used in this study is fluoride free composite, consists of barium glass fillers of 85 wt%. ClearfilTM SE bond is a fluoride free two step self etching primer adhesive system.6
In the present study, new coronal radicular technique is used a long with recently introduced packable composite i.e. Ormocer, to evaluate the fracture strength. In coronal radicular technique 2mm of the canal filling material is removed from the canal orifice and replaced with restorative material.4 Few studies have been conducted using this technique to check its efficacy.
This in vitro study is another effort to check the fracture resistance of endodontically treated maxillary premolar teeth with or without coronal radicular technique, and comparison among fracture resistance of various restorative groups and application techniques.
METHODS AND MATERIALS
Forty two freshly extracted human maxillary first premolars of nearly equal dimension were used in this study.. The samples were cleaned free of debris and calculus and were stored in humidity at room temperature. All the teeth were mounted in self cure acrylic resin to the level 2mm below the CEJ and the cusp tips alined in the same plane to ensure a more equal distribution of load during testing.
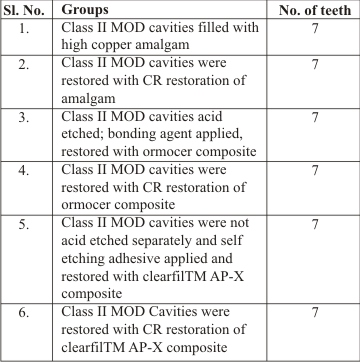
The teeth were randomly divided into six groups of teeth.
Table 1 : 42 teeth divided into 6 groups
 | Table 1 : 42 teeth divided into 6 groups
 |
TOOTH PREPARATION:
The cavity preparation and the method of restoration was standardized for all groups. Forty-two extracted human maxillary first premolars without caries were used in this study. Access cavities were prepared, two canals located, buccal and palatal. The root canals were enlarged to the apical foramen with K-files to size 50. A standard flare was done by the insertion of # 2 to # 5 gates glidden drills. Irrigation during cleaning and shaping was performed using a 2.5% NaOCl solution. After instrumentation all teeth were obturated with gutta percha and zinc oxide engenol sealer, by lateral condensation technique.
Then the teeth were randomly divided into six groups of 7 each. MOD cavities were prepared in each tooth down to the canal orifices making the buccal cusp of 2mm width at the occlusal surface and 3mm at the CEJ. (figure 1)
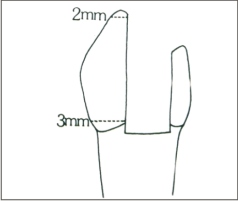 | Fig 1
|
In 21 specimens, 2 mm of the canal filling material was removed from the canal orifice with the help of gates glidden drill and replaced with restorative material. This technique is called coronal radicular restoration.
The teeth were restored in the following manner :
Group I: Tofflemire retainer and matrix band applied around the cavities and it is restored with high copper amalgam (DPI alloy), carved and polished after 24 hours.
Group II : In this 2mm of canal filling material was removed with gates glidden drill and after application of tofflemire retainer and band, amalgam was condenced, carved and polished after 24 hours. Teeth were restored with coronal radicular restoration of amalgam.
Group III : Cavities were acid etched with 37% of phosphoric acid for 15 seconds rinsed for 10 seconds and dried gently. A one layer of single bond (Admira, Voco) was then applied, and cured for 20 seconds with light curing unit having intensity of 450 mW/cm2. A steel matrix was applied with a tofflemire retainer. Ormocer composite was incrementally placed and cured. Each increment was cured for 40 seconds. The cavities were then contoured, finished (super snap kit) and polished with composite polishing kit.
Group IV : 2mm of canal filling material was removed with the help of gates glidden drill and cavities were restored with coronal radicular restoration of ormocer as described earlier.
Group V : Self etching primer coat was applied to the cavity walls, gently blew with the air and dried for 15 seconds. Single coat of adhesive was applied and light cured for 20 seconds with a light curing unit (Confident, India) having light intensity 450mW/cm2 (radiometer). A steel matrix was applied with a tofflemire retainer. The cavities were restored with ClearfilTM AP-X composite incrementally. Each 2mm increment was cured for 40 seconds. The cavities were then contoured, finished and polished with super snap kit and composite polishing kit (Shofu Japan).
Group VI : 2mm of canal filling material was removed with gates gildden drill and cavities were restored with coronal radicular restoration of ClearfilTM AP-X composite as described earlier.
TESTING
The restored teeth were stored in an incubator at 370 C in 100% humidity for 48 hours. Stainless steel custom made jig was made of angulations 150 degree. The teeth were tested with Instron Universal testing machine. Jig was fitted on the testing machine and samples were mounted in the polymethylmethacrylate. Directly the mounted samples one by one placed on the angulated platform of the jig and the buccal walls of the premolars were then subjected to slowly increasing force (1mm/min) at the junction of the buccal cusp and the filling material. The force was applied at a 150 degree angle to the long axis of the teeth. (figure2) The data were analyzed using a one way analysis of variance and Tukey test.
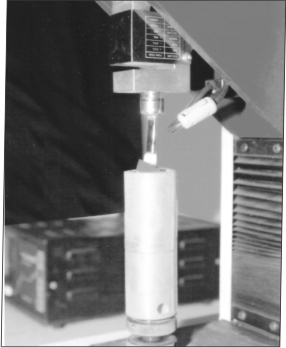 | Fig 2
|
RESULTS
The aim of the present study was to check the fracture resistance of endodontically treated premolars by various restorative materials.
Intragroup comparison – Unpaired t test
Intergroup comparison – One way ANOVA followed by Tukey’s hoc test pair wise comparison.
Force required to fracture individual endodontically treated tooth in each group, mean of each group and standard deviation are presented in following tables.
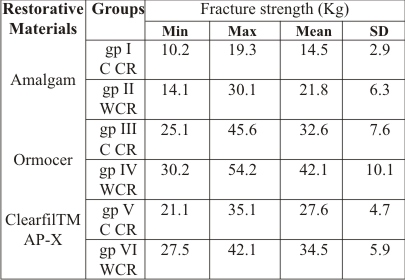
Table 2 : Load required to fracture teeth of different groups :
 | Table 2 : Load required to fracture teeth of different groups
|
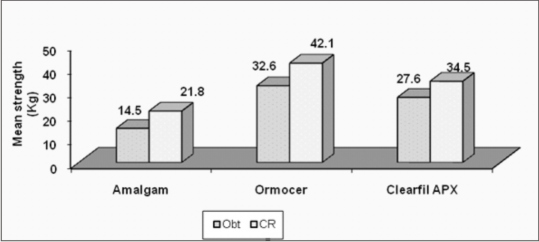
Graph 1. Means and standard deviation of different groups
 | Fig
|
Table 3 : Comparison of load required to fracture between various restorative materials and application techniques.
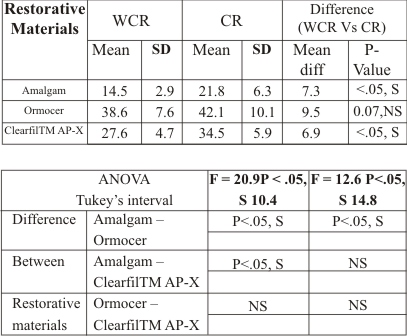 | Table 3 : Comparison of load required to fracture between various restorative materials and application techniques
|
One-way analysis of variance indicated a significant difference among the mean of groups. Tukey multiple comparison test revealed statistically significant differences among the mean of different groups. No statistically significant differences were found among the two application techniques for Ormocer. However, statistically significant differences were noted among the two application techniques for Amalgam and ClearfilTMAP-X.
Under the conditions of the present study, the tooth coloured restorative materials enhanced the fracture resistance of endodontically treated teeth, when coronal radicular application technique was used.
DISCUSSION
With inception of new materials, operative dentistry has undergone sea change. In addition to preservation of tooth, restoring the tooth strength to physiologic level has been the unequivocal goal. Composite resin bind micromechanically to tooth structure by forming resin tags and thus reinforce the tooth.22
It was concluded in the experiment that the width of the occlusal portion of preparation affects the strength of the crown of a prepared tooth. The extension of a preparation to involve proximal boxes does not significantly reduce the strength of a tooth provided only a minimal amount of dentin is removed.24 Preparation of mesioocclusodistal cavity where in two marginal ridges are crossed results in 35% decrease in fracture resistance of vital tooth.25
One of the most important controversial topics is how to reinforce the endodontically treated posterior teeth after mesiooclusodistal cavity preparation. It was found that endodontic treatment resulted in only a 5% reduction in the relative stiffness of a tooth, while on additional MOD preparation increased its value to 63%.9
More recently emphasis has been placed on intra coronal strengthening of teeth to protect them against fracture.14Today many different types of techniques and materials are available to better reinforce the endodontically treated tooth.
With the recent advancements in adhesive technology with stronger composite materials, it is possible to create highly aesthetic restorations that are bound directly to teeth. The resin forced into these tubules holds the tooth together, increasing its resistance to fracture.30 Study have shown that there is increase in the structure resistance of teeth, when MOD preparations were acid-etched before restoration with a composite resin.1
Admira, an Ormocer organically modified ceramic, packable composite used in this study consists of 3- dimensionally curing co-polymers of inorganic and organic elements, similar to tooth substance. It also contains an inorganic backbone of silicon dioxide and dimethacrylate as a resin base have filler size of 0.8ƒÝm and 82% by weight. Hybrid composite clearfilTM AP-X used in this study is fluoride free composite. ClearfilTM SE bond is a fluoride free two step self etching primer adhesive system. Composite consists of barium glass fillers of 85 wt%. An acidic monomer, 10-methacryloxydecyl dihydrogen phosphate (MDP), is present in the primer, which demineralizes the smear layer and underlying dentin, resulting in mild surface etching.6
The advantage of two step self etching adhesive system is that, it is a time saving procedure and there is no over wet and dryness of dentin after rinsing and drying because separate acid etching step is omitted.30
In the present study, new coronal radicular technique was used along with recently introduced packable composite i.e. Ormocer, to evaluate the fracture strength. Very few studies have been conducted using this technique to check the efficacy of this. Hence the aim of present study was to evaluate and compare the fracture resistance of endodontically treated teeth with two application techniques, with or without CR extension.
The difference between the height of the two cusps is more pronounced in the upper first than in the second premolar, and the occlusal slope of the facial cusp of the upper first premolar is more susceptible to fracture than the lingual cusp.33 Hence the fracture resistance was checked on maxillary first premolars and load was applied on the interface of buccal wall and restorative material.
The results showed that the specimens restored with coronal radicular restoration of Ormocer had better fracture resistance. Group (IV, VI) which were restored with coronal radicular extension of composites showed better fracture resistance than groups III and V restored with composite resin without coronal radicular extension. And the groups I and II which were restored with and without coronal radicular extension of amalgam showed less fracture resistance than rest of the groups.
These results suggest that teeth that are etched, bonded and restored with resin composite, the cusps are mechanically splinted together. The reaction of these teeth to a load is similar to the reaction of unprepared teeth. The cuspal reinforcing effect of bonded resin composite restorations has generally been accepted.34
Force required for groups. Group IV where Ormocer was used with coronal radicular technique showed maximum 42.1Kg of fracture strength i.e. highest among all the groups due to separate etching step and extension of bulk of restorative material into the root canal space, offers the additional resistance form to the pulp chamber.13
Group VI which was restored with ClearfilTM AP-X hybrid composite with coronal radicular technique showed less fracture strength that is 34.5 kg than group IV. ClearfilTM AP-X composite showed less fracture resistant values than Ormocer. The self-etching primers (SEPs) in this include a phosphonated resin molecule that performs two functions simultaneously, etching and priming of dentin and enamel. Unlike conventional etchants, self etching primers are not rinsed off, and when the surface was observed under scanning electron microscopy, shallower etching pattern was seen than when a conventional acid etchant was used.30 It consists of barium glass fillers which has a degradation rate higher in saliva simulating solutions. From a clinical viewpoint, using silica filled composite has been recommended instead of a glass – filled composite that leaches more filler elements and degrades faster.36 As the comparison was done by statistical analysis between Ormocer and ClearfilTM AP-X, P value was more than 0.05, which is not significant.
Group III that was restored without CR extension of Ormocer showed 32.6 kg fracture strength as compared to group V, which showed fracture strength of 27.4 kg and was restored without CR extension of Clearfil TM AP-X. Due to total etch system and presence of high filler loading, Ormocer showed better fracture resistance than ClearfilTM AP-X. Statistically when both the techniques with or without CR extension was compared for Ormocer, P value showed non-significant result. But for Clearfil TM AP-X, P values were less than 0.05, which is significant.
Group II restored with CR extension of Amalgam showed 21.8 kg fracture strength than Group I, which was restored without CR extension of Amalgam showed least fracture strength that is 14.1 kg. Statistically the P value for Amalgam with and without CR extension was less than 0.05, which is significant. In this study Amalgam restored teeth found to be less fracture resistant than packable composite and hybrid composite. This result is not surprising because traditional Amalgam restorations do not provide a tooth strengthening effect, but only bulk replacement of lost tooth tissue. On the contrary, they may act as wedge between the buccal and lingual cusps and therefore increase the risk of cuspal fracture. Condensation of Amalgam leads to cuspal deflection and this creates a strain in restoration on tooth complex thus reducing the fracture resistance of tooth.4
When restoring with composite many factors may affect the resistance of a tooth to vertical and/or cuspal fracture, such as cavity dimension or restorative system utilized. High visocity bonding agents may also provide a layer of substantial thickness that acts as a stress absorber.34
Strengthening effect on the teeth by the restorative materials is influenced by bond between restoration and tooth structure and modulus of elasticity of the restorative material.22,34
Composites have a lower modulus of elasticity (16.6 GPa) compared to Amalgam (27.6 GPa); therefore, more loads is absorbed in the composite resin than the Amalgam. Composite, therefore, may transmit less of the applied load to the underlying tooth structure.37 The continually increasing load applied to teeth in this study is not typical of the type of loading that occurs clinically. Except for a single traumatic incidence, teeth that crack or fracture in the mouth usually do as result of repeated episodes of stress that fatigue the crystalline structure and produce microcracks that propogate until failure of the structure occurs. Long term clinical trials are needed to assess these factors and to determine the longevity of different restorations and their usefulness in reducing the incidence of tooth fracture.
CONCLUSION
Following conclusions can be drawn from this study:
Packable composite, Hybrid composite do strengthen the endodontically treated tooth better than Amalgam, because the cusps are mechanically splinted together.
Coronal radicular technique gives better resistance to the material as compared to without coronal radicular technique, as it increases the bulk of material in the root canal.
Bonding ability of restorative systems to cavity walls is more effective when the preparations are separate acid etched before restoration.
REFERENCES
1. Belli S, Erdemir A, Ozcopur M, Eskitascioglu G. The effect of fibre insertion on fracture resistance of root filled molar teeth with MOD preparations restored with composite. Int Endod J 2005; 38: 73 –80.
2.Nagasiri R, Chitmongkolsuk S. Long-term survival of endodontically treated molars without crown coverage: A retrospective chort study. J Proshet Dent 2005; 93: 164 –70.
3. Trope M, Tronsad L. Resistance to fracture of endodotnically treated premolars restored with glass ionomer cement or acid etch composite resin. J Endodon 1991; 17(6): 257-59.
4. Hurmuzlu F, Kiremitci A, Serper A, Altundasar E, Siso SH. Fracture resistance of endodontically treated premolars restored with ormocer and packable composite. J Endodon 2003; 29(12): 838 – 40.
5. Karl FL, Stephen CB, Edward JS. Packable composite: over view and technical considerations. J Esthet Dent 1999; 11 (5): 234-49.
6. Tschiya S, Nikaido T, Sanoda H, Foxton RM, Tagami J. Ultrastructure of the Dentin – Adhesive Interface after acid – base challenge. J Adhes Dent 2004; 6: 183-90.
7. Bakke JE, Duke ES, Morling BK, Windler S, Mayhewer B. Fracture strength of class II preparations with posterior composite, J Den Res 1985; 64 (3); Abst No. 1578: 350.
8. Trope M, Maltz D, Langer I, Transtad L. Resistance to fracture of restored endodontically treated premolars. J Dent Res 1985; 64 (3); Abst No. 1231: 311.
9. Oliveira F de C, Denehy GE, Boyer DB. Fracture resistance of endodntically prepared teeth using various restorative materials. J Am Dent Assoc 1987; 115: 57-60.
10. Wendt Jr SL, Harris BM, Hunt TE. Resistance to cusp fracture in endodontically treated teeth. Dent Mater 1987; 2: 232 – 35.
11. Reeh ES, Messer HH, Douglgass WH. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J endodon 1989; 15 (11): 512-16.
12. Hansen EK, Asumussen E, Christainsen NC. Invivo fractures of endodontically treated posterior teeth restored with amalgam. Endod Dent Traumatol 1990; 6: 49-55.
13. Kane JJ, Burgess JO, Summitt JB. Fracture resistance of amalgam coronal – radicular restorations. J Prothet Dent 1990; 63: 607 –13.
14. Hernandez R, Bader S, Boston D, Trope M. Resistance to fracture of endodontically treated premolars restored with new generation dentin bonding systems Int Endod J 1994; 27: 281 – 84.
15. Linn J, Messer HH. Effect of Restorative procedures on the strength of endodontically treated molars. J Endodon 1994; (10): 479-85.
16. Costa LCS, Pegoraro LF, Bonfante G. Influence of different metal restorations bounded with resin on fracture resistance of endodontically treated maxillary premolars. J Prothet Dent 1997; 77: 365-9.
17. Steele A, Johnson BR. In vitro fracture strength of endodontically treated premolars. J Endodon 1999; 25 (1): 6 –8.
18. Assif D, Nissan J, Gafni Y, Gordon M. Fracture resistance of teeth with Class II bonded amalgam and new tooth colored restorations. J Proshet Dent 2003; 89: 462–5.
19. Yamada Y, Tsubota Y, Fukushima S. Effect of restorations method on fracture resitance of endodontically treated maxillary premoarls. Int J Prosthodont 2004; 17: 94 –98.
20. Grandini S, Goracci C, Tay FR, Grandini R, Ferrari M. Clinical evaluation of the use of fiber posts and direct resin restorations for endodontically treated teeth. Int J Prosthodont 2005; 18: 399 – 04.
21. Mannoccif, Qualtrough AJE, Worthington HV, Watson TF, Pittford TR. Randomized clinical comparisons of endodontically treated teeth restored with Amalgam or with fiber posts and Resin composite: 5 year results. Oper Dent 2005; 30 (1): 9-15.
22. Jagadish S, Yogesh BG. Fracture resistance of teeth with Class II silver amalgam, posterior composite and glass cermet restorations. Oper Dent 1990; 15 (2): 42 –7.
23. Craig RG, Powers JM. Restorative dental materials. 11th ed. St Louis (Missouri): Mosby. Publishers; 2002.
24. Larson TD, Douglas WH, Geistfeld RE. Effect of prepared cavities on the strength of teeth. Oper Dent 1981; 6: 2-5.
25. Marzouk MA, Simonton AL, Gross RD. Operative Dentistry, Modern theory and Practice. All India Publishers; 2001.
26. Phillips science of Dental Materials, 11th ed. St Louis (Missouri): mosby.. Publishers; 2002.
27. Trope M, Maltz DO, Tronstad L. Resistance to fracture of restored endodontically treated teeth. Endodent Traumatol 1985; 1: 108-11.
28. Leinfelder KF, Barkmeier WW, Goldberg AJ. Quantative measurements of posterior composite resins. J Dent Res 1983; 62: 71.
29. Roulet JF. The problems associated with substituting composite resins for amalgam: a status report on posterior composites. J Dent 1988; 16 (3): 101 –13.
30. Roberson TM, Heymann HO, Swift EJ, JR. Sturdevants art and science of operative dentistry. 4th ed. St Louis (Missouri): mosby. Publishers; 2002.
31. J Leinfelder KF, Rotz GM, Nash RW. A report on a new condensable composite resin. Compendium 1998; 19 (3): 230 –37.
32. Perry R, Kugel G, Leinfelder K. One-year clinical evaluation of Surefil packable composite. Compendium 1999; 20 (6): 544-53.
33. Mansen EK. Invivo cusp fracture of endodontically treated premolars restored with MOD amalgam or MOD resin fillings. Dent Mater 1988; 4: 169-73.
|