Introduction
An impression which is the negative registration of ridge and border tissues accomplished by one or more impression materials. It is a record of these tissues taken while at rest or in a displaced position.
Four basic principles/fundamentals of impression making which the prosthodontist seeks to achieve are – 1.Area coverage, 2.Periphery, 3.Valve seal without interference with functional movements 4. Accurate adaptation to the tissues without injurious displacement.(1)
One of the important parts of impression making is the preliminary mouth examination which should include a complete radiographic survey, visual & digital examination, & a notation of the patients denture history.(2)
Using a stock metal tray which will afford full coverage of the denture bearing area, a primary compound impression of the arch is made. To make an acceptable primary impression, certain anatomic landmarks must be visible such as the residual ridge, retromolar pads, external oblique ridges including the buccal shelves, mylohyoid ridges & the labial and sublingual gland portions of the ridge.
Case Report
A 85 year old male patient visited the Department of prosthodontics crown and bridge, Peoples college of dental sciences & Research Centre, Bhopal with the chief complain of an ill fitting upper denture since 2 years. The patient was a denture wearer for the past 15 years; within this span his denture was replaced twice. Medical history revealed that there was no underlying systemic disorder.
On Examination intra oral examinations revealed a flabby anterior ridge extending from canine to canine region (Fig 1) and completely resorb lower ridge (Fig 2). A treatment plan of fabricating a complete denture with the modification in the impression technique to achieve minimum displacement of denture during function and maximum retention and stability.
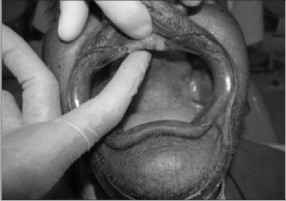 | Fig 1 Upper Flabby ridge
 |
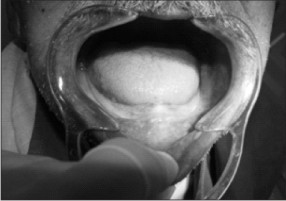 | Fig 2 Completely resorb lower ridge
|
Material And Method
After an acceptable primary impression is secured (Alginate : Dentsply, wey bridge Surrey, U.K), the impression is boxed with a patty of plaster and pumice. This prevents the plaster from flowing into the lingual area of the plaster cast which is made for the purpose of constructing an individual acrylic tray.
The finished plaster cast is outlined to an approximate 2 to 3 mm under extension from the extension anticipated in the finished denture. This under extension should afford sufficient space for muscle trimming the borders. Anatomic landmarks that will prove helpful in outlining the cast are the retromolar pads, external oblique ridges and mylohyoid ridges.
One thickness of baseplate wax is adapted & cut to this penciled outline, quick curing acrylic is prepared & adapted to the wax shim on the plaster cast, after 20 minutes the acrylic tray is removed from the cast & trimmed to the outline of the wax shim, at this time a compound handle can be constructed for the tray.
The individual tray with the wax shim attached is tested in the mouth for 2-3 mm under extension, then the wax is removed from the tray.
Reason for making initial impression & special tray constructed are –
The tray filled with soft impression compound is much easier to center on the cast than in the patients mouth.
A more even pressure may be applied while centering the tray.
The tray should be reglazed & seated in the mouth to aid in tissue adaptation.
The tray is then muscle –trimmed with impression compound, section by section to provide maximum denture bearing area it is recommended that maximum coverage of the buccal shelf should be attained but within limits of tissue tolerance. Full extension of the denture borders with in tissue tolerance, is recommended for the lateral throat form area.
Maximum extension here will aid materially in the lateral stability of the denture.
The finished compound muscle trimmed (border moulding) impression (DPI Pinnacle tracing sticks) is then carried to the mouth & tested for proper extension. Proper extension is interpreted as being muscle trimmed to the borders tissues, yet not interfering with these normal movements or functions.
The wax which has been used for the spacer is then removed to allow space for the impression .Impression is taken with Zinc Oxide Eugenol paste (DPI Impression paste, Mumbai) ; the impression tray is guided to position rather than forced into place.
In order to aid in the insertion of the tray, the patient is instructed to touch the roof of the mouth with the tip of the tongue upon its initial insertion. Only enough finger pressure is maintained to ensure the proper position of the impression tray. No muscle trimming is done at this time, as the original muscle-trimmed border has been preserved.
The finished impression is ready, now a no: I5 B.P. blade is used to scrape out the part of the impression covering the flabby ridge area, once area is scrapped & clean, light body ( ZhermackR Clinical Oranwash-L impression material) rubber base impression is mixed & loaded in the area of the flabby ridge & the impression tray is again reseated in the patients mouth.
The impression now obtained (Fig 3) is properly boxed & poured with a thick mix of stone. The cast obtained is used to fabricate a special tray in the similar manner as earlier, and on this new special tray is fabricated , the final wash impression (Fig 4) is taken using –
Light body
Medium body ( ZhermackR Clinical Thixoflex-M impression material )
Elastomeric/rubber base silicone impression materials (Fig 4)
This results in a nice wash impression of the flabby ridge including the remaining residual ridge & surrounding areas with high degree of accuracy & then the denture is carried to completion.
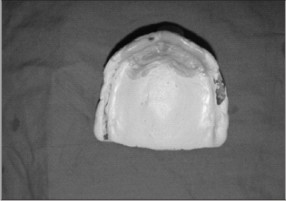 | Fig 3 Impression with zinc oxide eugenol and light body
|
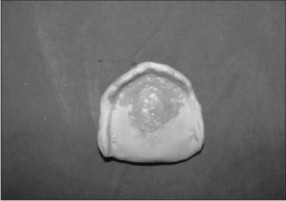 | Fig 4 Final impression with light and medium body
|
The exact reproduction of the ridge tissue is most important to the patient not only for comfort but also because it will provide maximum denture base adaptation & will allow perfect adhesion by contact.
DISCUSSION
Managing a patient with a flabby maxillary ridge can be challenging problem and taking care to consider the influence of both the impression surface and occlusal surface detail in paramount. Standard muco-compressive impression techniques are likely to result in an unretentive and unstable denture as the denture constructed on a model of the flabby tissue in a distorted state. The use of selective pressure or minimally displacive impression techniques should help to overcome some of these limitations. The use of holes, windows and wax relieve reduces the hydraulic pressure and minimize the displacement of the bearing tissues. The suggested two methods eliminates them excessive displacement of the soft tissues at the secondary impression thus a physiologic and anatomic registration of the attached and the unattached tissue of the denture bearing areas are attained. (3,4)
This article describe the impression technique to minimally displace the flabby tissue and reproduction of maximum details. Choice of treatment modality is made by keeping in mind that the requirement of stability and retention of the prosthesis must be balanced along with the preservation of the health of oral tissues for every patient.
Summary & Conclusion
All the denture bearing areas within the limits of tissue tolerance has been covered, not the residual ridge alone but the most important buccal shelf and retro molar pad as well.
Peripheral extension – Peripheral borders have been established within the limits of tissue tolerance.
Valve seal – without interference with functional movements; by establishing a periphery which harmonizes with the anatomic and physiologic landmarks surrounding the denture, this provide good valve seal but also maximize lateral stability.(5)
Accurate adaptation to the tissues without injurious displacement and a final wash impression of the tissues , provides accurate adaptation without injurious displacement and equal distribution of stress.
There must be no displacement of tissues and if some amount of displacement accurs it must be minimum so that the elastic force is is not greater than the retentive force.
There must be intimate contact between the denture base and the undisplaced tissue for adequate retention for the management of the flabby ridge.(6)
References
1) Watson RM: Impression technique for maxillary fibrous ridge : Br Dent J 1970; 128: 552
2) Tallgreen A : The continuing reduction of the residual alveolar ridges in complete denture wearers a mixed longitudinal study covering 25 years : J Prosthet Dent 1972 ; 27 ;120-132
3) Allen F: Management of the flabby ridge in complete denture construction : Dent Update 2005; 32: 524-528
4) Kelly E: Changes caused by a mandibular removable partial denture opposing a maxillary complete denture. J Prosthet Dent 1972; 27: 140-150
5) Lynch CD and Allen PF. Management of the flabby ridge: using contemporary materials to solve an old problem. Br Dent J 2006; 200:258-261.
6) W. Chee and S. Jivraj :Treatment planning of the edentulous mandible. British Dental Journal (2006); 201, 337-347 |