INTRODUCTION
The term Early Childhood Caries (ECC) was suggested at a 1994 workshop sponsored by the Centers for Disease Control and Prevention.1The American Academy of Pediatric Dentistry defines Early Childhood Caries(ECC) as the presence of one or more decayed (non-cavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary teeth in a child of 71months of age or younger. In children younger than 3 years of age, any sign of smooth-surface caries is indicative of severe early childhood caries (S-ECC). From ages 3 through 5, 1 or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing, or filled score of 4 <(age 3); 5<(age 4); or 6<(age 5) surfaces constitute S-ECC.2
Several factors important in the development of the decay are: repeated exposure, the duration of a feeding habit (times per day, during the day or night, and the age of the child), microorganisms, the time of tooth eruption, and the structure and defense mechanisms of the tooth3 and temperament of a child.4,5 Nursing caries is commonly associated with an inappropriate feeding habit of the infant. Not only bottle abuse (mostly containing sweetened beverages) but also prolonged breast feeding is considered to be a contributing factor to the development of caries in early childhood. Under normal dietary conditions, milk is not considered to be cariogenic agent, but repeated and prolonged exposure leads to a larger decrease in plaque pH.3 Natural fruit juices and, particularly, sweetened fruit drinks, soft drinks, contain significant concentrations of sugar and their improper use in infant feeders also may cause dental decay. There is growing concern today that a similar result may occur from giving sweetened medications in feeding bottles to infants and young children.6 These pharmaceutical preparations have a mean sugar content of 55% to make them more palatable and to mask the unpleasant taste of drugs, especially for children. 7
A strong correlation has also been found between oral hygiene habits and the prevalence of caries. The more the brushing is performed, the less caries children experience.8
Children who have caries in their primary teeth in infancy or as toddlers tend to develop additional dental decay in their primary teeth and are more likely to develop caries in their permanent teeth after they erupt. Therefore, the most important target group for instituting preventive programs seems to be infants and toddlers.1
Despite of several studies done on ECC worldwide, not much data is available on the prevalence of ECC and the associated risk factors in the preschool children of Haryana, particularly in Gurgaon. Hence, the present study, was undertaken with the following aims and objectives:
a) to determine the prevalence of Early Childhood Caries,
b) to assess the associated risk factors which include inappropriate and prolonged feeding habits, improper tooth brushing habits, administration of sweet based medication and temperamental variations in urban preschool children in Gurgaon, Haryana and,
c) Follow up for dental health assessment(caries & oral hygiene) after 3 months in caries active children.
MATERIAL AND METHODS
SELECTION OF SAMPLE
Study sample comprised of 702 children of both sexes from age group 2 to 6 years from 5 kindergarten schools of Gurgaon, Haryana. The selection of sample was random. A structured questionnaire was sent to the parents of the children through their class teachers before conducting the study. The form included the information about their child's vital statistics, parental education status, their dishes of interest, feeding habits, tooth brushing habits, administration of sweet based medication and the temperament of the child as rated by their parents.
Only those children were finally included in the study which had been examined and of those whose completed questionnaires were returned. Thus, the final sample consisted of 600 children only. The research protocol of the survey was reviewed and permission was obtained from Ethics Board Committee of the institution. A prior consent for the dental examination of the child had been taken from the parent as well as from the school authorities.
Dental Examination
Children were visually examined in their respective classrooms by one examiner under daylight or a torch light. The examiner was trained and pre-calibrated in the Department of Pedodontics and Preventive Dentistry, SGT Dental College, Gurgaon. No radiographs were taken for any child. The examination was done at random without the prior knowledge of the findings of the questionnaire. A plane mouth mirror and a dental explorer were used. Diagnosis depended upon visual evidence of a lesion, the explorer was only used to remove plaque or food debris and not to confirm or refute doubtful diagnosis. Sterilized instruments and separate gloves were used for each patient. Caries status of the child was recorded using deft index (Gruebell,1944) on a specially designed proforma. Oral hygiene status of a child was also evaluated as mentioned below (using specially designed criteria):
GOOD- Clean teeth with no signs of debris
FAIR- Traces of soft white deposits with stains
POOR- Abundance of soft matter and food lodgment and stains.
Motivational pamphlets were handed over to the children that included the required preventive measures of early childhood caries. The purpose was to give information to the parents about their child’s oral health status and preventive measures available for them.
A follow up examination was performed after three months only for the caries active children. Caries status was noted again on the same standardized proforma.
Data thus obtained was entered in an MS-Excel spreadsheet and analyzed using Chi-square test to determine the association between ECC and various risk factors.
RESULTS
Out of the 600 children, 332 were males and 268 were females. Four age groups were formed for the data analysis: Group I: 24-36 months; Group II: 37-48 months; Group III: 49-60 months and Group IV: 61-72 months.
The mean deft was found to be 2.85. All the deft was mostly due to untreated caries. The overall caries prevalence was found out to be 68.7%.(Table 1)
The habit of inappropriate feeding practices (night feeding with bottle) was present maximum in Group II (53.7%), and least in Group IV (45.3%).Thus, the overall prevalence of children with inappropriate feeding habits especially at night is 52% (Table 2). A significant increase was found in dental caries experience in children with bottle feeding habit especially at night (P < 0.001).
The temperament of the child was classified as difficult or easy going. Difficult temperament was present more in group II (26.16%) than in group IV (20.9%) and the overall prevalence of children with difficult temperament was 25.3% proving a significant association between dental caries and children with difficult temperament (P < 0.001) (Table 2).
Good oral hygiene was found the maximum in group I (65.1%) and least in Group IV (48.8%) providing a significant relationship between increased caries experience and improper oral hygiene (P < 0.001).
Group II (16.4%) had the maximum children consuming sweetened medication routinely and least in group IV as 12.7% but a significant relationship was found between dental decay and consumption of sweetened medication frequently (P< 0.001).
After 3 months follow up, decayed teeth (dt) and filled teeth (ft) were again recorded on a specially designed proforma for 185 caries active children. It was found that mean dt at baseline was 3.95 which reduced to 1.57 after three month follow up and mean ft recorded at baseline was 0.15 which got increased to 2.69 after three months of dental checkup.
DISCUSSION
Dental caries is a complex disease, the cause of which has received significant attention during the nineteenth and most of twentieth century.9 The Centre for Disease Control & Prevention reports that caries is perhaps the most prevalent infectious disease in our nation’s children. More than 40% of children have caries by the time they reach kindergarten. Early Childhood Caries can be a particularly virulent form of caries, beginning soon after tooth eruption, developing on smooth surfaces, progressing rapidly, and having a lasting detrimental impact on the dentition.10 In our study, the final sample comprised of 600 children studying in various kindergarten schools of Urban Gurgaon in age group of 2-6 years fulfilling the criterion of definition given by AAPD1. Our study targeted children belonging to middle class families having a sound socioeconomic status as several studies have been conducted using similar variables in rural set up.11,12,13,14 Thus, this study targeted the preschool children as children in age group of 2-6 years were easily accessible.15
The 'def index' was described by Gruebbel16 as an equivalent index to DMF index, for measuring dental caries in primary dentition.17,18 No attempt was made to use a dental probe to confirm catch of the lesions due to the young age of the children. This ensured their compliance with the examination without adversely affecting their cooperation and behavior in the dental environment in future. Moreover, studies have quoted that the use of probe disrupts the surface layer and prevents the possibility of reversing the non cavitated through remineralization.19,20 A specially designed criterion was used to grade the oral hygiene status of the children. It was made for easy applicability in younger children. The status was divided into three classes such as good, fair and poor. A child’s oral hygiene was graded as good when the teeth were clean having no signs of debris, as fair when traces of soft white deposits and stains were present and was referred as poor when abundance of soft matter and food lodgment was present. It was mainly based on visual inspection.
In our study, the mean deft recorded was 2.85 which was higher than the findings reported by Tewari & Tewari12 in Rohtak, Haryana. They reported the average deft as 2.37. The low caries experience of decayed teeth might be attributed to the fact that this study was carried out in the peri urban areas of Rohtak. As most of the population in rural area preferred underground water than the centralized water supply, hence, there would have been more consumption of fluoride in drinking water which may result in resistance against caries.12 Another study conducted in Ludhiana city (Punjab) by Simratvir et al 19 also reported lower mean caries score of 1.86. The reason attributed would be that in this study, caries diagnosis was entirely based on visual inspection, this certainly resulted in an underestimation of the caries status. We also relied mainly on visual inspection but periodontal probe was used in cases of food lodgment. Various studies worldwide have reported a higher dental caries experience than ours study. One such study in South Africa conducted by Cleaton-Jones et al reported a high dental decay score of 3.7 in preschool children. The reason could be that they used probes for all children whereas we relied mainly on visual inspection. Therefore, this could have altered the results of the study.21
In our study, mean deft in the youngest age group 2-3 years was lowest recorded as 2.55 and highest in the age group 3-4 years as 3.11. Mean deft values in age groups 4 to 5 years and 5 to 6 years were also high recorded as 2.77 and 2.98 respectively. Similar results have been reported in study by Simratvir et al19, Kaste et al22 & Mohebbi et al.23 The caries experience has been found to increase from age group 2-3 years to 5-6 years. This may be partly due to increased consumption of sugar containing food24,25 and/ or change in dietary habits.19 The higher caries experience at 6 years of age was in agreement with other studies.26,19 In our study, the overall prevalence of early childhood caries was high recorded as 68.7%. Similar results have been reported in the literature18,26,27,28 while Tyagi29 found 19.2% prevalence of nursing caries in Davengere preschool population. The prevalence of dental caries has been found to be variable as follows: 70%, 53%, 25%, 50.8%, and 51.46% in the age group of 5-6 years in Bangalore (Urban), Davangere (Urban), Davengere (Rural), and Kerala (Rural) respectively.30 The reason for such high caries prevalence could be that most of the children were under supervision of caretakers or domestic help rather than parents themselves. Also it was observed that all the kindergarten schools provided sweet-based foods everyday as an additive snack in between meals.
In our study, the overall prevalence of children with inappropriate feeding habits especially at night was 52%. Similar results have been reported by many authors.8,31 The reason stated could be that inappropriate feeding practices offer a favorable medium to bacteria growth, restricts salivary flow and formation of acid plaque. This plaque determines the reduction of oral pH and induces the demineralization of enamel and may lead to cavity formation. Stagnation of milk at the level of anterior teeth and lactose dizaharide fermentation lead to caries formation.32,33
In our study, the overall prevalence of children exhibiting difficult temperament was 25.3%. A significant relationship was found between temperament of a child and Early Childhood Caries in our study. A difficult temperament was exhibited by 32.5% of caries active children. In a study conducted by Quinonez et al5 reported that shyness and inability to socialize attributes of a child’s temperament were associated with Early Childhood Caries. The reason may be attributed to the fact that difficult temperament has been linked with feeding and sleeping difficulties. It has been found that children with difficult temperament are not easy to put to sleep at night therefore, to pacify them bottle may be used.
In our study, the overall prevalence of children lacking oral hygiene was 46.3%. Compromised oral hygiene was found in 59% caries active children. Similar results were reported by Tewari & Tewari 13, Stecksen and Holm 34, Leverett et al 35and Vanobbergen et al.8
In our study, the overall prevalence of children on frequent use of sweetened medication was found to be 15.5%. 21.4% of caries active children out of the sample were found to be on frequent use of sweet based medication on routine basis. A significant increase was found in dental caries experience in children with regular use of sweetened medication. In vitro studies have shown the demineralizing potential of iron tonics, effervescent vitamin preparations, proprietary mouth rises, and medicines used in the treatment of phenylketonuria.36 It has also been stated that sugar containing medications with prolonged oral clearance gets metabolized by bacteria to acid end products, lower pH within bacterial plaque that is unavailable to salivary buffering. Low pH causes ionic dissolution from the hydroxyapatite crystals, leading to enamel and dentin demineralization. Diminution of salivation and lack of mastication movements during the night increase the cariogenic potential of medicines.7
The dental check up after three months was only conducted for the caries active children after patient and parent motivation. Out of 412 caries active sample, 185 children were present on the day of dental check up. The reason for such low follow up sample was attributed to the fact that some children in the older age group of 5 to 6 years had left the kindergarten school after three months and the rest were absent for the dental check up. Baseline and follow up values of decayed and filled teeth were compared for those 185 children. It was found that mean decayed teeth (baseline) was 3.95 which got reduced to 1.57 after three months follow up and the mean filled teeth (baseline) score recorded was 0.15 which got increased to 2.69 after three months.
CONCLUSION
The prevalence of ECC was 68.7% in urban Gurgaon preschool children. A significant increase in dental caries was present in children with inappropriate feeding habits, improper oral hygiene, difficult temperament of a child and frequent use of sweetened medication.
LIMITATIONS OF STUDY
The survey was done only in five schools. This might have biased the study results, as the sample taken is not representative of the population.
Only frank cavitated lesions were only included. This might have led to underestimation of results.
 | Table 1 Mean deft and Caries Prevalence in various age groups
 |
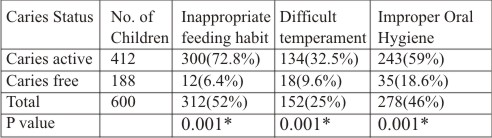 | Table 2 Association between caries experience and various risk factors
|
REFERENCES
1. Horowitz HS. Research issues in early childhood caries. Community Dent Oral Epidemiol. 1998; 26(1): 67-81.
2. American Academy of Pediatric Dentistry. Pediatric Dentistry.2009; 31(6): 13-13(1).
3. Weerheijm KL, Uyttendaele-Speybrouck BFM, Euwe HC, Groen HJ. Prolonged Demand Breast-Feeding and Nursing Caries. Caries Res. 1998; 32: 46-50.
4. Tiberia MJ, Milnes AR, Feigal RJ, Morley KR, Richardson DS, Crof WG et al. Risk factors for early childhood caries in Canadian preschool children seeking care. Pediatr Dent. 2007; 29(3): 201-208.
5. Quinonez R, Santos RG, Wilson S, Cross H. The relationship between child temperament and early childhood caries. Pediatr Dent. 2001; 23(1):5-10.
6. Twetman S, Garcia-Godoy F, Geopferd SJ. Infant Oral Health. Dent Clin North Am. 2000; 44(3):487-505.
7. Bigeard L. The Role Of Medication And Sugars In Pediatric Dental Patients. Dent Clin North Am. 2000; 44(3):443-456.
8. Vanobbergen J, Martens L, Lesaffre E, Bogaerts K, Declerk D. Assessing risk indicators for dental caries in the primary dentition. Community Dent Oral Epidemiol. 2001; 29:424-34.
9. Sofowora AC, Nasir WO, Taiwo M, Adesina OA. Caries experience in the primary dentition of nursery school children in Ile-Ife, Nigeria. African Journal of Oral Health. 2006;2:19-25.
10. American Academy Of Pediatric Dentistry. Guidelines on Infant Oral Health. Pediatr Dent (Reference Manual).2010/11;32: 114-118.
11.Kuriakose S, Joseph E. Caries prevalence and its relation to socio-economic status and oral hygiene in 600 pre-school children of Kerala-India. J Indian Soc Pedo Prev Dent.1999;17;97-100.
12.Tewari S, Tewari S. Caries experience in 3-7 year old children in Haryana (India). J Indian Soc Pedo Prev Dent.2001;19: 52-56.
13.Jose B, King NM. Early childhood caries lesions in preschool children in Kerala, India. Pediatr Dent.2003;25:594-600.
14.Saravanan S, Madivanan I, Subashini B, Felix JW. Prevalence pattern of dental caries in the primary dentition among school children. Indian J Dent Res. 2005; 16:140-6.
15.Dhar V, Jain A, Van Dyke TE, Kohli A. Prevalence of dental caries and treatment needs in the school going children of rural areas in Udaipur district. J Indian Soc Pedo Prev Dent. 2007; 25:119-121.
16.Gruebbel AO. A measurement of dental caries prevalence and treatment service for deciduous teeth. J Dent Res. 1944;23:163-8.
17.Hegde SK, Kumar KBS, Sudha P, Bhat SS. Estimation of salivary bacteria capable of inhibiting and stimulating Streptococcus mutans, and its correlation to dental caries and untreated carious teeth. J Indian Soc Pedod Prev Dent.2005;23:126-130.
18. Leake J, Jazzy S, Uswak G. Severe Dental Caries, Impacts and determinants among children 2-6 years of age in Inuvik region, Northwest territories, Canada. J Can Dent Assoc.2008;74:519-519g.
19.Simratvir M, Moghe GA, Thomas AM, Singh N, Chopra S. Evaluation of caries experience in 3-6 year old children, and dental attitudes amongst the caregivers in the Ludhiana city. J Indian Soc Pedo Prev Dent. 2009; 27: 164-169.
20.Hamilton JC, Stookey G. Should a dental explorer be used to probe suspected carious lesions? J Am Dent Assoc. 2005;136:1526-32.
21. Cleaton-Jones P, Richardson BD, McInnes PM, Fatti LP. Dental caries in South African white children aged 1-5 years. Community Dent Oral Epidemiol.1978;6:78-81.
22.Kaste LM, Selwitz RH, Oldakowski RJ, Brunelle JA, Winn DM, Brown LJ. Coronal caries in the primary and permanent dentition of children and adolescents 1-17 years of age:1988-1991. J Dent Res (Spec iss)1996;75:631-41.
23.Mohebbi SZ,Virtanen JI,Golpayegani MV,Vehkalahti MM. Early Childhood Caries and dental plaqueamong 1-3 year olds in Tehran,Iran. J Indian Soc Pedod Prev Dent.2006; 24 : 177-181.
24.Kalasbeek H, Verrips GH. Consumption of sweet snacks and caries experience of primary school children. Caries Res.1994;28:477-483.
25.Holm AK. Caries in preschool child:International trends. J Dent. 1990;18:291-5.
26.Jamieson LM, Thomson WM, McGee R. Caries prevalence and severity in urban Fijian school children. International J Pediatr Dent. 2004;14:34-40.
27. Namal N.,Vehit H.E.,CanG. Risk Factors for dental caries in Turkish children. J Indian Soc Pedod Prev Dent.2005; 23: 115-118.
28. Carino KMG, Shinada K, Kawaguchi Y. Early childhood caries in northern Philippines. Community Dent Oral Epidemiol. 2003; 31:81-9.
29.Tyagi R.Prevalence of nursing caries in Davengere preschool children and its relationship with feeding practices and socioeconomic status of the family. J Indian Soc Pedod Prev Dent.2008; 26: 153-157.
30.Mahejabeen R, Sudha P, Kulkarni SS, Anegundi R. Dental caries prevalence among preschool children of Hubli: Dharwad city. J Indian Soc Pedod Prev Dent. 2006; 24:19-22.
31.Kelly M, Bruerd B. The Prevalence of Baby Bottle Tooth Decay Among Two Native American Populations. J Pub Health Dent. 1987;47:94-97.
32.Pasareanu M. Considerations regarding early childhood caries. J of Preventive Medicine. 2007;15:130-133.
33.Bowen WH. Response to Seow: Biological mechanisms of early childhood caries. Community Dent Oral Epidemiol. 1998;26(supl 1):28-31.
34.Stecksen-Blicks C, Holm A.K. Between meal eating, toothbrushing frequency and dental caries in 4-year-old children in the north of Sweden. International J Pediatr Dent. 1997; 19: 67-72.
35.Leverett DH, Featherstone JDB, Disney JA, Adair SM, Eisenberg AD, Mundorff-Shrestha SA et al. Caries risk assessment by a cross sectional discrimination model. J Dent Res.1993; 72:529-37.
36.Maguire A, Baqir W, Nunn JH. Are sugar free medicines more erosive than sugar containing medicines? An in vitro study of pediatric medicines with prolonged oral clearance used regularly and long term by children. International J Pediatr Dent. 2007; 17: 231-238.
|