INTRODUCTION:-
Within the last 20 years, diagnostic digital modalities in dentistry, including periapical, bitewing, panoramic and cephalometric imaging, have been replacing conventional (filmbased) radiography. Drawbacks of two-dimensional (2-D) imaging include inherent magnification, distortion and overlap of anatomy. As early as the 1920s, manufacturers attempted to overcome the problems of 2-D imaging by devising movement of the source and
receptor in opposite directions to produce tomographic “slices” of oral and maxillofacial anatomy; this process is termed as “linear” or multidirectional tomography” which led to the introduction of micro CT (computed tomography), CBCBT, (Cone beam computed tomography), OCT(Optical coherence tomography) and “ Tuned aperture tomography”(TACT). These techniques are as follows:-
Computed Tomogaphy uses a fan shaped beam and multiple exposure around an object to reveal the internal architecture of the object. In this way the clinician can view the morphological features as well as pathology from different three dimensional perspectives. However, if ratio opaque materials are present, there can be scattering and creation of artifacts which can significantly hamper visualization.1
Cone Beam Computed Tomography(CBCT) orVolumetric CT a relatively new diagnostic imaging modality, has been used in endodontic imaging recently. This modality uses a cone beam instead of a fan shaped beam acquiring images of entire volume. It offers high resolution , isotropic images for effective evaluation of root canal morphology.2
Optical Coherence Tomography is a new diagnostic imaging technology that was first introduced in 1991.3OCT combines the principles of an ultrasound with the imaging performance of a microscope. OCT uses infra red light waves that reflect off the internal micro structure within the biological tissues. Using the principle of low –coherence interferometery it achieves depth resolution of the order of 10ìm and in plane resolution similar to the optical microscope. By scanning the probe along the imaged specimen while acquiring image lines, a two dimensional or three dimensional image is built up
Tuned Aperture Computed Tomography (TACT) is a flexible 3D imaging method that converts any number of 3D projections produced from any number of arbitrary or even unknown projection source positions and angles into a true 3D image. The image produced is similar to viewing the original object with unlimited visual access through a window or aperture whose size is determined by the original projection. Such 3D displays could be useful for caries/ demineralization detection and in the determination of root fractures especially vertical fractures.Three dimensional technology enables reconstructions, with suitable enhancement and refining of the digital image, form upto 7 images of the region of interest at different angles. At the moment the development of TACT in dentistry is centered on using a panoramic system as the radiation source.4,5,6
Ultrasonography With Color Doppler
Ultrasonography can give an idea about the nature and dimension of lesion which helps in pre-operative assessment and treatment planning.7,8
How ever, here we are discussing the most commonly used techniques and presenting case reports in relation to them.
Computed Tomogaphy
CT endodontic applications were first reported by Tachibana and Natsumoto in 1990.9 They reported that CT had only limited usefulness in endodontics as a result of inadequate image detail and a high cost. However one distinct advantage of CT is that it allow for 3-D construction of root canal systems (RCSs).10 3D information along with tactile feedback during instrumentation gives the clinician more understanding of true
morphology of RCSs.
Some CT software programs add colour enhancement features to highlight pathological lesions from normal anatomic structures. CT images have the ability to show the slices of the given tissue, with each tissue thickness and location chosen by the operator. Therefore CT would enable the operator to look at the multiple slices of tooth roots and there RCSs.1 CT has been suggested as the preferential imaging modality in difficult situations demanding localistaion and description of RCSs because of its ability to render 3D information.11
Micro CT has been evaluated in endodontic imaging. Comparison of the effects of biomechanical preparation on canal volume on reconstructed root canals in vitro using micro CT shown to assist with characterization of morphological changes associated with these techniques.12,13
Micro CT imaging of filled root canals showed it to be a highly accurate and non destructive method of evaluation of root canal filling and their constituents. Qualitative and quantitative correlation between histological and micro CT examination of root canals filling was high.13,14
CT may play an important role in optimizing palatal root end surgery through vestibular access, with regards to precision and preventing complications, with relatively low biological and economic cost, also possibly contributing to the affirmation of the new procedure.12Ebihara et al incorporated with 3D construction in the diagnosis and monitoring of the case of Garres’s osteomyelitis managed by root canal treatment of a mandibular 2nd molar.15
Traditional radiographs could only determine the mesiodistal extent of the pathology and not the buccolingual extent16.trope et al in 1989 for the first time used CT scans for the differentiation of radicular cysts and granulomas. A cyst could be differentiated from the periapical granuloma by CT scans because of marked difference in density between the contents of the cyst cavity and granulomatous tissue.17
A major concern with the use of CT scan is its high radiation dosage. In a study18 guidelines by Cristoph et al19were use, using these guidelines, effective radiation dosage reduced by this method was 0.56+/-0.06mGy, which was equivalent to a standard panoramic radiograph. The result of the study indicate that CT scan and ultrasound with power Doppler flowmetry can provide additional or alternate but more accurate diagnosis of periapical lesion with validity equivalent to histopathological diagnosis.
CT used to evaluate root canals prepared by nickel titanium(NITI)hand and steel hand endodontic instruments showed that the system used in the study provided a repeatable no invasive method of evaluating certain aspects of endodontic instrumentation.20
CASE REPORT WITH SPIRAL CT :
This report presents two cases of diagnosis of radix entomolaris and detection of mesiobuccal two (MB2) canal in retreatment case by spiral computerized tomography. In both the cases strict adherence to ALARA(as low as reasonably achievable) principle of radiation dose were maintained.
Case Report
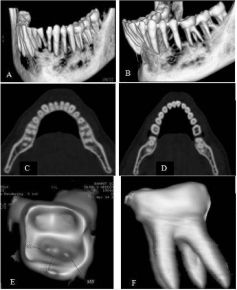
A 23 year old male patient reported to the Department of Conservative Dentistry and Endodontics, Seema Dental College & Hospital, Rishikesh with a complaint of severe tenderness on biting pressure. Intraoral periapical radiograph revealed a small carious lesion in the distal surface of right mandibular first molar (46) with a periodontal pocket of 3.5mm probing depth. Two outlines of distal roots are appreciated on a digital radiograph captured with Kodak CCD software. After obtaining a written consent from the patient a mandibular plane spiral CT (SOMATOM, ACCULITE SOFTWAE) was done with a pitch of 0.05mm. Spiral
CT images clearly shown a distoloingual root (Radix entomolaris) in the involved tooth.
 |
 |
Figure 1: IOPA X- RAY
Figure 2 : EXTRA DISTOLINGUAL ROOT
Figure 3: SHOWING EXTRA DISTOLINGUAL ROOT IN 46.
Ultrasonography With Color Doppler
Ultrasound with a colour Doppler is a proven, useful and non invasive diagnostic tool in endodontics. Periapical lesions accompanying endodontic infection are usually diagnosed and treated based on the initial radiological findings.21 Sometimes periapical surgery is necessary to eliminate and diagnose the cystic and non cystic nature of the lesion.
CASE REPORT WITH COLOR DOPPLER AND ULTRASONOGRAPHY Case Report :(FIG 4-9)
A 22 yr old male patient reported to the department of conservative dentistry and endodontics with a chief complaint of pain and swelling in maxillary anterior region. Periapical radiograph showed a large radioluscent area in the region of 21, 22.
An ultrasound examination was performed using the diagnostic ultrasound machine, HLS 9ED SONOACE 8000 LIVE*/ EX PRIME (Medison America Inc. USA) with color doppler function, incorporating a high definition, multifrequency ultrasonic Probe ( 3D 3 5EK probe ) operating at a frequency of 0.60KHz (90 decibel). The probe position was changed in order to obtain transverse scans (axial plane) and longitudinal; scans (saggital plane).
Colour Doppler was applied to detect internal vascularisation. The image was analysed by an expert ultrasonographer. A tentative differential diagnosis of periapical granuloma was agreed upon based upon the following principles.22
Granuloma: a poorly defined hypoechoic area, showing rich vascular supply on colour Doppler examination.
Cystic lesion: a hypoechoic well – contoured cavity surrounded by reinforced bone walls, filled with fluid and with no evidence of internal vascularisation on colour Doppler examination.
Mixed lesion : predominantly hypoechoic area with focal anechoic area, showing vascularity in some areas on colour Doppler Examination.
Following conventional principles of periradicular surgery the case was operated and biopsies were obtained from the periapical areas.10,11,12,13,23,24 Result of the biopsy was found to be a periapical granuloma as confirmed by ultrasound and colour Doppler.
 |
|
FIG 4- PREOPERATIVE PHOTOGRAPH
FIG 5- IOPA RADIOGRAPH TOOTH NO 21,22 WITH PERIAPICAL LESION
FIG 6-ULTRASONOGRAM IN 21,22 REGION
FIG7- ULTRASONOGRAM WITH COLOUR DOPPLER SHOWING VASCULARISATION
FIG 8- 3D RECONSTRUCTED IMAGE OF GRANULOMA
FIG 9 – HISTOLOGICAL REPORT SHOWING GRANULOMATOUS TISSUE
CONCLUSION :
Several advanced radiography techniques for the precise detection of the lesions and root canal systems have been in use in endodontics, namely digital radiography, CBCT, OCT, CBCT, ultrasound etc. The use of novel imaging techniques is gaining a lot of attention in the field of endodontics but the need of the hour is to develop a cost effective chair side three dimensional imaging system for routine use..
References-
1. Brooks SL. Computed tomography. Dent Clin North Am 1993:37;575-90.
2.Nair MK,nair UP, Digital and advanced imaging in endodontics, a review. J Endod, 2007 , 33;1-6
3.Huang D,Swason EA, Lin CP et al. Optical coherence tomography . Science 1991;254;1178-81
4.Webber RL, Messura JK. An in vivo comparison of diagnostic information obtained from tuned aperture computed tomography and conventional dental radiographic imaging modalities Oral SUrg Oral Med Oral Pathol Oral Radiol Endod 20203;96:223-8.
5. Nance R, Tyndall D, Levin LG. Identification of root canals in molas by tuned aperture computed tomography.Int Endod J 2000;33:392-6.
6.Nair MK, Nair UDP, Grondanl HG. Et al.Detction of artificially induced vertical fractures using tuned aperture computed tomography. Eur J Oral Sci 2001;109:375-9.
7. Cotti E, Campisi G, Ambu R , Dettori C. Ultrasound real time imaging in differential diagnosis of periapical lesions. Int Endod J 2003;36:556-563.
8. Cotti E, Campisi G, Garau V, Puddu G. Anew technique for the study of periapical bone lesion: ultrasound real time imaging. Int Endod J 2002;35:148-152
9. Tachibana H, Matsumutu K. Applicability of X-ray computerized tomography in endodontics.Endod Dent Traumatol 1990;6:16-20.
10. Dowker SEP,Davis GR,Elliot JC.X-ray microtomography:non destructive three dimensional imaging for in vitro endodontic studies.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:510-6.
11. Robinson S, Czerny C, Gahleinter A , Bernhart T et al .Dental CT evaluation of mandibular first premolar root configurations and canal variation. Oral Surg Oralmed Oral Pathol Oral Radiol Endod 2002;93:328-32.
12. Rigolone M, Pasqualini D,Bianchi I et al . Vestibular surgical access to the palatine root of superior first molar . “ low dose cone beam CT ananlysis of the pathway and its anatomic variations.” J Endod 2003;29:773-5.
13. Jung M, Lommel D, Klinek J. The imaging of root canal obturation using micro-CT. Int Endod J2005;38:617-26.
14. Gullaume B, Lacoste JP, Gabroit N, et al. Micro computed tomography used in the analysis of morphology of root canals in extracted wisdom teeth.Br J Oral Maxillofac Surg 2006;44:240-4.
15. Ebihara A, Yoshioka T, Suda H. Garre’s osteomyelitis managed by root canal treatment of mandibular second molar: incorporation of computed tomography with 3D reconstruction in diagnosis and monitoring of the disease. Int Endod J 2005;38:255-61.
16. Kaffe I, Gratt BM. Variation in radiographic interpretation of periapical dental lesions. J Endod 1988;14:330.
17.Trope M,Pettigrew J, Petras J et al. Differentiation of radicular cyst and granuloma using computerized tomography. Endod Dent Traumatol 1989;5:69-72
18. Agarwal V, Logani A, Shah M. Evaluation of computed tomography scans and ultrasound in the differential diagnosis of periapical lesions. K Endod 2008:34:1312-32.
19. Christroph GD, Wilfried Gh Britta R et al. Must radiation dose for CT of maxilla and mandible be higher than that for the panoramic radiography? Am Soc Neuroradiol 1996;96:1709-58.
20. Gambill Jm, Alder M,del Rio Ce:Comparison of NiTi and Stainless stell hand file instrumentation using computed tomography.J Endod 196;22:369-75 .
21. Gundappa M, Ng SY, Whaites EJ. Comparison of ultrasound digital and conventional radiograohy in differentiating periapical lesions.Dent max fac Radiol 2006;35:326- 333.
22. Nielsen AB; Alayssin AM, Peters DD, Carnes DL, Lancster J, microcomputed tomography: an advanced system for detailed endodontic research. J Endon 1995; 21; 561-8.
23. Rigolone M, Pasqualini D,Bianchi I et al . Vestibular surgical access to the palatine root of superior first molar . “ low dose cone beam CT ananlysis of the pathway and its anatomic variations.” J Endod 2003;29:773-5.
24. Velvart P, Hecker H, Tilinger G. Detection of apical lesion and mandibular canal in conventional radiography and computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92:682-8.
|