INTRODUCTION
Limited mouth opening (microstomia) can be defined as a reduction in the perimeter of the oral cavity or an abnormally small orifice. In healthy individuals mouth opening is around 30-50mm. But when the mouth opening is limited to a maximum of 20mm, the individual is said to have a reduced mouth opening. Limited mouth opening in itself is not a disease but manifests as a consequence of certain conditions, namely, surgical treatment of oro-facial carcinomas, cleft lip, trauma and burns, Plummer-Vinson’s syndrome, scleroderma, trismus, temporomandibular joint dysfunction syndrome, rheumatism, oral submucous fibrosis, or any damage to the masticatory muscles. Scleroderma is a disease that causes fibrosis by affecting the connective tissue and the blood vessels; it is believed to stem from a disorder of the immune system. Oral sub-mucous fibrosis is a pre-cancerous condition, chronic in nature, highlighted by fibrous transformation of juxta-epethelial layers which lead to mucosal rigidity & inability to open the mouth. Salivary secretion decreases due to tissue dehydration.
A maximal oral opening that is smaller than the size of a complete denture can make prosthetic treatment challenging. Several techniques have been described for use when either standard impression trays or the denture itself becomes too difficult to place and remove from the mouth. The literature contains reports on the fabrication of a foldable, hinged posterior section with molar and premolar teeth and a second denture base on which anterior teeth were arranged. Sectional dentures have been recommended, with the denture pieces connected by clasps. McCord et al10 described a maxillary complete denture consisting of 2 pieces joined by a stainless steel rod with a diameter of 1 mm fitted behind the central incisors.
During a prosthodontic procedure, it is the loaded impression tray that forms the bulkiest item requiring intraoral placement. This, compounded by the presence of limited mouth opening, makes the task of obtaining a proper path of tray placement a difficult and challenging procedure. In this article, a different design for the fabrication of mandibular and maxillary sectional trays is described. The technique was used for a patient whose oral opening was limited as a result of oral submucous fibrosis.
CLINICAL REPORT
An edentulous lady, 65 years of age, had reported to the clinic with chief complaint of inability to open the mouth. (fig 1, 2) Her masticatory function was normal (fig 1, 2). She was suffering from this condition from last one year. On investigation it was found that she had some decayed teeth which were painful, and to suppress that she was advised to use tobacco and slowly it became a habit. All the decayed teeth were extracted later.
 |
 |
Fig-1
Fig-2
EXTRA ORAL EXAMINATION
It revealed decreased lower facial height, decreased mouth opening only 2.5cm from upper lip to lower lip, toughened lips, restricted TMJ movement, with class III profilerelation.
INTRA ORAL EXAMINATION
Examination revealed severely resorbed lower ridge except for the canine to canine area. (Atwood classification class IV in mandibular and class III in maxillary arch). The cheek mucosa was taut. The tongue was large and the mouth was dry. Mucosa was pale and shining with a thinned soft palate, and an ill defined posterior palatal seal.
IMPRESSION PROCEDURE
The smallest trays were tried but failed to enter into the mouth. So impression compound (Y-Dent, MDM Corp. India) was kneaded and shaped approximating to the ridge shape and countered and loaded on the ridge at bearable temperature and impressions completed in both arches and cast were poured with type II dental plaster. (Neelkanth, India)
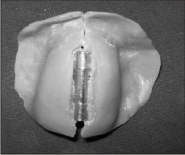
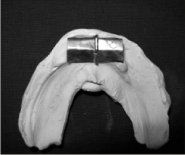
Maxillary special tray fabrication
A steel door hinge of length 20 mm, breadth 4 mm and a thickness of 1.5 mm) was selected. The preliminary cast was marked with lead pencil to give guidelines for the placement of the hinge. Cold mould seal was painted on the tissue surface of the cast. Using sprinkle- on method, auto- polymerising resin (RR, Dentsply, India) was sifted approximately to 2mm thickness. Two vertical locators were made on the outer surface of the tray over the ridge for cross- arch stabilisation and stabilized by a flat piece of wooden plank which was also used as handle. A vertical cut was made in the midline near the labial frenum, incisive papilla, mid-palatine raphe and posterior palatal seal area, so as to enable a folded special tray technique and tray was completed. (fig 3, fig 4)
 |
|
Fig-3
Fig-4
ular special tray:
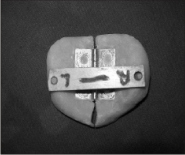
A hinge was made with 2 aluminium sheets of 16 mm length, 12mm breadth, and 0.5 mm thickness. Strip ‘A’ was taken moulded on the left side of the arch, to approximately 3 mm length and breadth. The centre part of the sheet was slit & the outer areas were folded towards the sheet where a metal wire was inserted which formed the centre of axis of the hinge. Strip ‘B’ was taken and moulded on the right side of the arch. The side were slit with approximately 3mm length & breadth leaving a central portion extending out.
This was folded towards the sheet with the wire in the centre which was fixed in strip A & the hinge was finished (fig 5). Cold mould seal was painted on the tissue side of the cast and the hinge was placed on the cast & auto polymerising resin was added onto it using sprinkle-on-method to approximately 2mm thickness. The tray was slit in the midline near the labial frenum, ridge and lingual frenum without damaging the metal part. The tray is now foldable to ease entry of it into the oral cavity. A small handle was constructed on the left side of the midline of the ridge and it helped in seating the tray perfectly on the ridge (fig 6).
Fig 5
Fig-5
Fig-6
FINAL IMPRESSION
Maxillary arch:
On the maxillary special tray, tray adhesive (Dentsply)was applied and medium body silicone (Reprosil, Dentsply Caulk, USA) was used in single step technique to take the impression of the border areas. After that the tray was loaded with impression material and placed in the in the oral cavity, once the left side of the tray was placed on the ridge, the right side was unfolded and pressed against the right side of the patient mouth. The tray was further stabilised by wooden stabiliser and border moulding was completed in single step (fig 7, 8). The tray was then removed from the patient mouth and a slit was made in the mid-line with BP blade (no 3) where the hinge was present to make the tray foldable. Polyvinylsiloxane light body material (Reprosil Dentsply Caulk, USA) was loaded on the tray and same procedure as above was followed to stabilise and make the master impression. And it was removed from the mouth without any difficulty.
Fig-7
Fig-8
Mandibular arch:
The tray adhesive was applied to the mandibular special tray and single step tray moulding was done using R.W. Tench technique for impression for impression. Medium body material (Reprosil, Dentsply, Caulk USA) was loaded on to the tray and taken into the mouth in a folded fashion. First the tray was seated onto the left side, then using the handle the tray was unfolded and seated into the right side of the arch and border moulding was completed (fig 9). Then the tray was removed and slit was made in the hinge area and the light body polyvinylsiloxane material (Reprosil Dentsply Caulk, USA) was loaded on the tray and inserted in same way as above mentioned. Impression was completed and removed with tray unfolded and master cast were made. (fig 10)
Fig-9
Fig-10
JAW RELATIONS AND TEETH ARRANGEMENT
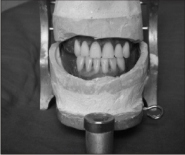
Occlusal rims were made with shellac base plate (Pyrex, India) and modelling wax sheet (Y dent no 2, MDM Corp, India). Jaw relation record was made at reduced vertical dimension in static method with Niswonger’s technique (fig 11). The patient exhibited a class III jaw ridge relation. The occlusal rims were fused in the mouth and taken out. Mounting of the cast & occlusal rim were done on a mean- value articulator. Teeth election was done (Acry Rock, Ruthinium) and arrangement was done in class III, edge- to- edge relationship in anterior region (fig 12). Second
premolars were omitted from all four quadrants; the teeth were set in cross bite in posterior segment to increase stability and denture try-in was done.
Fig-11
Fig-12
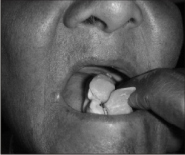
The denture was fabricated with Ivoclar-Triplex material and extensions of all margins were checked for rough margins and they were polished and finished. Denture adhesive was applied on the tissue surface of the complete denture and inserted in the mouth. Initially, the patient had difficulty to place and remove the denture comfortably. But after 3-5 weeks she was able to carry out these manoeuvres comfortably Fig 13
Fig-13
DISCUSSION
Many methods have been tried to fabricate dentures for patient with restricted mouth opening. This effort was an indigenous idea to create a collapsible tray and make impression and fabricate the prosthesis for a patient who was suffering from oral submucous fibrosis. This technique shares disadvantages common to all sectional tray/prosthesis designs, namely, additional time, labor, and materials. However, todetermine the long-term success of this technique, periodic recall, maintenance, and further improvements in design are needed.
CONCLUSION
The patient who comes with a debilitating problem should be mentally prepared about the possible outcome of the limitations. Sincere efforts should be done both by the dentist and the patient at every stage so a functionally acceptable prosthesis can be attained as a success of our hard work.
REFERENCES
1. Acuri M.R, Elike L, Deets K, maxillary sectional tray technique for microstomia patients; Quintessence dental Technol 1986;10:627-9.
2. Cura C, Cotert Hs, User A; Fabrication of a sectional impression tray and sectional complete denture for a patient with microstomia and trismus: a clinical report. J Prosthet Dent 2003;83;540-3
3. Benetti R Zupi A, Toffanin A; Prosthetic rehabilitation for a patient with microstomia a clinical report. J Prosthet Dent 2004;92:322-27
4. Laith Abd, Hana Abas; Treatment of an edentulous patient with surgically induced microstomia: A Clinical report; J Prosthet Dent 2002;87;423-26
5. Philip S. Baker, Robert L Brandt; impression procedure for patient withseverely limited mouth opening; J Prosthet Dent 2000;84:241-44.
6. The glossary of prosthodontics 8th ed. J Prosthet Dent. 2005; 94:1-92.
7. Conroy B, Reitzik M. Prosthetic restoration in microstomia. J Prosthet Dent 1971; 26:324-7.
8. Al-Hadi LA. A simplified technique for prosthetic treatment of microstomia in a patient with scleroderma: a case report. Quintessence Int 1994;25:531-3.
9. Ohkubo, et al. Application of cast iron-platinum keeper to a collapsible denture for a patient with constricted oral opening: A clinical report. J Prosthet Dent 2003; 90:6-9.
10. McCord JF, Tyson KW, Blair IS. A sectional complete denture for a patient with microstomia. J Prosthet Dent 1989; 61:645-7. |