INTRODUCTION :
Both surgery and radiation therapy are used in treatment of Squamous cell carcinoma (SCC). If an adequate margin of normal tissue can be obtained, surgery is the usual treatment, followed by radiation treatment. Alternatively, radiation may be used as a primary treatment followed by surgery salvage. Radiotherapy can be applied by external beam also known as brachytherapy. 1, 2
Brachytherapy can be divided into multiple categories: Interstitial, intracavitary, intraluminal, and surface applicator techniques. In addition, the application can be further subdivided depending upon the loading technique (preloading or after loading), the dose rate (low dose rate [LDR] or high dose rate [HDR]), and duration of the implant (temporary or permanent). In interstitial brachytherapy, the radioisotope is placed temporarily or permanently either into the tumor site or into bed. Intracavitary or intraluminal brachytherapy entails temporary application in a natural cavity near the tumor bed. Surface application has been more commonly applied intraoperatively after a gross total resection to the exposed tumor bed while shielding adjacent normal tissues. 3
The purpose of present clinical report is to describe the procedure of fabrication of "brachytherapy radiation carrier appliance(BRCA)" for the treatment of early stage SCC'S of the mandibular anterior alveolus. The carrier has been fabricated from auto polymerizing acrylic resin. Radiation carrier that will be worn must be carefully constructed to provide maximum patient comfort and correct dose delivery to treatment area.
CLINICAL REPORT
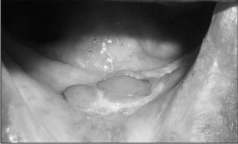
A 75 year old edentulous male was presented with a chief complaint of abnormal growth in lower front region of mouth since 3-4 months.(Fig 1) .On intraoral examination ,two nodular lesions in the region of anterior mandibular alveolar ridge (2 ×2 mm )and mucobuccal fold adjacent to It (3 ×4 mm) were observed . The biopsy of the lesion confirmed the diagnosis as SCC
Case was discussed with a radiation oncologist and brachytherapy with the aid of a BRCA was planned for the patient.
 |
 |
Fig 1. Preoperative photograph.
PROCEDURE Of FABRICATION Of APPLIANCE
1. Maxillary and mandibular impressions were made with modeling plastic impression compound using stock trays. While making mandibular impression the lip was pulled out and the impression prudently extended to cover the region of the neoplasm. Casts were prepared with dental stone. (Fig 2)
Fig 2. Definitive casts.
2.After fabricating the trial bases maxillomandibular relationship in vertical and horizontal planes were recorded and casts were mounted on a class II type A articulator. 4
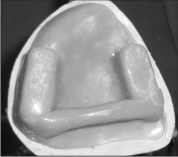
3. The appliance for the maxillary arch was fabricated with autopolymerising acrylic resin. The purpose of the maxillary appliance was to aid in the stabilization of the Mandibular appliance while the tongue was in position. To stabilize the tongue, an acrylic shaft was attached to the appliance.(Fig 3)
Fig 3. Maxillary appliance.
Fig 3. Maxillary appliance.
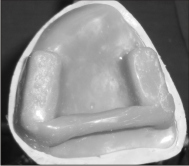
4. Mandibular appliance was fabricated with autopolymerising acrylic resin to cover the edentulous ridge along with the region of the lesion. (Fig.4) and both the appliances were tried in patient's mouth.(Fig 5)
Fig 4. Mandibular appliance.
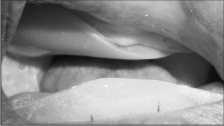
Fig 5.Appliance tried in patient's mouth for stability and comfort.
5. The exact positions for placement of the nylon radiation carrying tubes were planned after careful discussion with the radioncolgist. (Fig. 6)
Fig 6.Exact markings for nylon tube positioning.
6. 3 grooves of approx. 5 mm diameter were placed on the tissue surface of the appliance with the help of a round bur for the placement of nylon tubes which would transport the radioactive source to the target site. These grooves were placed approximately 1 cm distance from the margins and 1 cm from each other.
7. Nylon tubes were placed in grooves and secured in position with adhesive tape .
8. The appliance was tried in patient's mouth and checked for stability, position of the tubes and discomfort to the patient.(Fig. 7)
Fig 7 .Definitive appliance in the patient's mouth
DISCUSSION
The use of custom-made acrylic resin radiation appliance can be a valuable adjunct to the radiation treatment of oral cancers. Because the anatomical locations of the lesions are usually inaccessible, so to provide radiotherapy the carrier appliance should have good retention; stability and support. Retentive clasps can be incorporated in the appliance, if required.
The presented BRCA allows consistent and stable direction of a radiation beam for treating intraoral lesions5. As the plastic tubes are positioned at the predetermined exact location by physicist and oncologist, the close proximity
of the radiation source to the lesion radiation limits radiation scatter and helps assure a more constant beam to the radiation field thereby minimizing the side effects of radiotherapy. The delivery of radiotherapy through this appliance reduced discomfort of both oncologist and patient due to short immobilization period.
The presented procedure is a simple non-invasive procedure. Radiation exposure of treating and nursing staff is eliminated. In HDR, mold brachytherapy the radioactive source accurately positioned for the treatment of small lesion. The BRCA enables the radiotherapist to deliver a high dose of 50 Grays in 10 - 15 days. HDR mold brachytherapy eliminates the morbidity of surgery, preserving the function of salivary glands
The fabrication of splint for edentulous patient in two piece provide ease of placement by radiooncolgist and patient .Placement of rod shaped acrylic resin in posterior part of upper appliance help in positioning the tongue in its position. Hence, this appliance can be called as radiation carrier as well as position maintaining device.
Moreover, the technique for fabrication of BRCA requires materials that are readily available and there is no need of special prosthodontic expertise laboratory procedures or expensive equipments. Minimal clinical time is required and appliance can be given to the patient in a single visit, hence treatment of the patient is not delayed because of the minimal time required for the fabrication of the appliance.
SUMMARY
The principles of fabricating an intraoral radioactive carrier have been described to treat malignant disease of oral cavity .The prosthesis provides consistent direction and fixation of radioactive source into the same location.
REFERENCES
I. Adisman K , Desjardins R P. Use of the afterloading technique for intraoral radiation carriers. J. Prosthet. Dent.1985; 53:676 -678.
2. Shafer, Hine, Levy, Textbook of oral pathology. 5thedition p.161.
3. Anupama Sharma, Kenneth S. Kurtz, Kenneth M. Schweitzer, David R. Silken & Jonathan Beitler, A customized orofacial brachytherapy carrier: A clinical report. J. Prosthet. Dent. 2005; 93:24 -27.
4. Winkler S, Essentials of complete denture prosthodontics.2nd edition.p.142-154
5. Beumer J, Curtis TA, Marnick M T.Maxillofacial rehabilitation: Prosthodontic and surgical considerations. St. Louis: Medico dental media Intl Inc; 1979. p. 23 - 40
|