INTRODUCTION
The highly resorbed residual ridge is the scourge of prosthodontist's. Swenson stated, "The ideal ridge is one that is broad on its bearing surface and has practically parallel sides"1. Seldom are these encountered by prosthodontist's. Deterioration of this ideal ridge is frequently accomplished before it exists, because of multiple factors, which may be local or systemic2. So the patients presenting with severe ridge resorption are relatively common today both in private office and teaching institutions. It is the poor retaining and supporting alveolar situation. The greatly increased maxilla-mandibular space further complicates the problem. Our objective is to construct a stable and retentive prosthesis for the purpose of restoring aesthetic, function and tissue preservation. The purpose of this article is to discuss how this can be achieved.
A Case report:
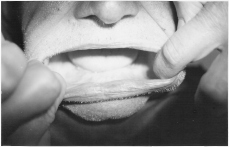
A 70 year old male patient reported to department of prosthodontics, H P Govt. Dental College Shimla with chief complaint of loose upper and lower completes denture and inability to masticate food. He repeated the complete denture several times but the results were unsatisfactory. On examination it was found that patient had highly resorbed upper and lower ridges (fig 1& 2), dentures were overextended, bases unstable with high vertical dimension of occlusion. A new denture was planned for this patient utilizing modified impression technique and occlusal scheme to construct a stable, retentive and well functioning prosthesis. Technique3:
 |
 |
Fig 1
Fig 2
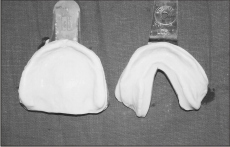
The main feature of this technique is that it makes use of selective tissue placement impression without the use of any wash material, for making final impression of the flat ridges. The basic principle4 is to utilize existing oral anatomy for the best results and prognosis. As stated by Sears "we do not take but we make impression" according to the needs of individual's oral cavity, taking into consideration anatomy, histology and physiology of the supporting and surrounding tissues to accommodate the tissues with variable degree of displaceability and form. The initial impression (fig 3) was made with
Fig 3
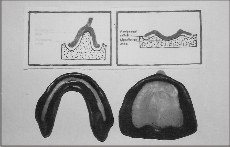
alginate in stock trays to capture the attached mucosa of the ridge crest with less tissue displacement effect. The primary casts were prepared from these alginate impressions. Autopolymerising acrylic resin (DPI India) special trays (fig 4) were prepared on primary casts giving relief on the peripheral borders and slopes of the ridges with single thickness of base plate wax. The peripheral borders of the special tray must be within 3mm of the desired denture periphery to adequately capture the peripheral sulcus area during border molding procedure.
The unrelieved portion of the tray was closely adapted to the primary cast while making special tray, as it is the final impression for that area and no impression material is placed over this area and also it act as a positive stop and seat during border molding procedure. Advantages of this technique are:
Fig 4
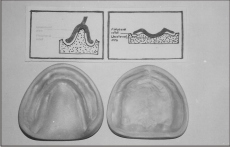
The relieved area of the tray was functionally border molded with impression compound to capture the movable tissues on the peripheral sulcus area and slopes of the ridges with additional tissue placement effect, as it is the primary supporting and stress bearing area. This functionally border molded tray was the final impression without the use of any wash material. Advantages of this technique are:
Fig 5
1. The degree of retention and stability can be positively predicted prior to the final completion and different areas may be built up and reduced to develop maximum retention and stability through the use of impression compound.
2. The unrelieved portion of the custom tray covers a large area, so it helps in proper placement of the tray in each insertion and provides better stability and support during border molding procedure.
3. The technique offers selective tissue placement impression without the use of any wash impression which saves the cost and clinical time also.
4. The custom tray is rigid, properly contoured for each patient and is practical to use.
The final casts (fig 6) were prepared from these functionally border molded (fig 5) trays and articulated on semi adjustable articulator after recording the vertical and horizontal jaw relation records.
Fig 6
Modifications6 made in the occlusal scheme were:
1. Incisal guidance was kept minimum taking into consideration aesthetics, phonetics and ridge relation.
2. 33° (anatomic) posterior teeth were used for maxillary denture to obtain the functional efficiency and 10° teeth were used for mandibular denture to prevent the locking of upper and lower denture during functional movements.
3. Bucco-lingual width of posterior teeth was decreased so as to decrease the force per unit area of the ridge.
4. Teeth were placed close to the base to prevent tipping leverage effect.
5. Lingualized concept of occlusion was used to increase the stability, comfort and to lingualize the occlusal forces.
After the trial, denture was fabricated and remounted on a semi adjustable articulator to refine the occlusion and then inserted.
POST INSERTION FOLLOW UP:
Patient was observed for one year in the post insertion phase with weekly appointments during 1st month and then regular appointments (three month appointment) up to one year. He was satisfied aesthetically as well as functionally.
 |
|
Fig 7
CONCLUSION:
The basic principle is how to utilize the existing oral anatomy for best results and prognosis. To achieve success nothing can replace good judgement coupled with knowledge of basic fundamental principles. Allen Brewer stated that any of the several techniques and material will work if we understand what we want to capture and create. We should modify our procedures to cope with the existing oral anatomy presented by each patient3. The technique used in this case was very helpful in patients with severe ridge resorption to construct a stable, retentive and well functional prosthesis.
REFERENCES:
1. Swenson M. complete denture. 2nd ed.st Louis. C V Mosby PII: 1947.
2. Douglas C Wendt. The degenerative denture ridge care and treatment. J Prosthet Dent1974; 477-89.
3. Alexander R Halperin. Mastering the art of complete denture. Quintessence; 1988: p 23-79.
4. Devan MM. basic principle of impression making. J Prosthet Dent 1952; 2-26.
5. Sears VH. Functional impression for rebasing full denture. J Am Dent Assoc 1936; 23:1031.
6. Desrajdins RP. Management of difficult lower denture. J Prosthet Dent 1974:32; 243.
7. Sheldon Winkler. Essentials of complete denture prosthodontics. 1996: 2nd ed: p 226-27.
8. Boucher. Prosthodontic treatment for edentulous patients.1997: 11th ed: p 141-82. |