INTRODUCTION:
In day to day dental practice it is observed that patient report only in case of pain and generally seen that tooth has already decayed so much that without proper diagnosis [3, 4, 5] a dentist advises root canal treatment and patient in
pain has no other option and hence get going. Now what if pain is persisting even after excellent root canal therapy and why is such a question that keeps the dentist in dilemma that why pain. Now importance of correct diagnosis and diagnostic aids come into play. Radioluecency seen at peri apical region of the root canal treated teeth is seen. In some cases infection persists or recurs around the root canal treated teeth. In such cases it becomes necessary to surgically intervene and assess the infection directly clean it around the tooth root hence “A Periodontist” [1, 2].
CASE REPORT
A 30 year female reported in the department of periodontology, with persistant complaint of dull pain and pus discharge i.r.t right maxillary central incisor (Fig.2). On clinical and radiographic evaluation after complete history was taken, it was found that she had undergone multiple root canal therapies for the treatment of the same complaint. Last root canal therapy was done 4 weeks ago. Radiographic examination revealed loss of lamina dura, lateral and periapical radioleucency surrounding the tooth root (Fig.1). Clinical examination revealed a probing depth of 7mm distal to right maxillary Central Incisor (C.I) (Fig.4), palatal probing depth was around 4mm. It was decided to surgically operate the area. Treatment plan was properly explained to the patient and a written consent of the patient was taken.
Local anesthesia sensitivity test was done (Fig.3) and then proper anesthesia was administered to the patient. Crevicular and vertical releasing incisions were made and full thickness mucoperiosteal flap was raised (Fig.5). After the
flap was raised it was visualized there was marked loss of alveolar bone around the root surface. The tooth was not mobile as the mesio and disto palatal bone was still intact (Fig.6). The defect was thouroughly debrided and irrigated (Fig.7) andwas followed by root conditioning and placement of Osseoconductive bone graft (Fig.8). Soft tissue
was approximated with 3-0 mersilk suture properly (Fig.9). Recall of the patient was done after one week for suture removal and then after 2 and 4 weeks respectively clinical and radiographic evaluation was done.
CONCLUSIONS:
Radioleucency was eliminated and trabaculae formation was seen (Fig 10, 11, 12). Apical periodontitis, which may be radiographically [7]
 | Fig. 1. Pre-OP Radiograph
 |
 | Fig. 2 Pre-OP (Sinus Opening with Pus Discharge)
|
 | Fig. 3 Sensitivity Test (Local Anesthesia)
|
 | Fig. 4 Probing Depth
|
 | Fig. 5 Incisions.
|
 | Fig. 6 Lesion Visible Clinically
|
 | Fig. 7 Debridement of the Lesion
|
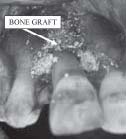 | Fig. 8 Bone Graft Placement
|
 | Fig. 9 Suturing after Bone Grafting
|
 | Fig. 10 Post Suture Removal (After One Week).
|
 | Fig. 11 Lesion Asymptomatic After 15 Days of Suture Removal.
|
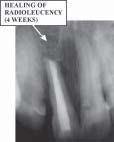 | Fig. 12 Post OP Radiograph (Post Suture Removal 4 Weeks)
|
undetectable or may be larger causing destruction to bone, is likely to persist or emerge in most root filled teeth as a consequence of residual endodontic post-treatment root infection. If the objective of root canal treatment is defined as
elimination of apical periodontitis at a histological level, current treatment procedures must be improved. At the same time, it is essential that further knowledge is acquired of the local and systemic biological consequences of residual post treatment root infection and post-treatment apical periodontitis.
REFERENCES:
1. Basnet P, Kamath MP, Kundabala M, Menda A Kathmandu University Medical Journal (2005), Vol. 3, No. 4, Issue 12,
415-417
2. Dr. Cheng Po Feng, DDS Perfect Dental® Newsletter: TAIWAN, JANUARY 2007
3. Nevin A et al. Metastatic carcinoma of mandible mimicking periapical lesion of endodontic origin. Endod Denz Traumatol, 1988;4: 238-239.
4. Cutler R. Neoplasia masquerading as periapical infection. Brit. Dent J 1990;168:348-349
5. Smith S. et al. Periapical cemental dysplasia: a case of misdiagnosis. Brit. Dent J 1998;185:122-123
6. Horner K. Film fault artefact mimicking periapical radiolucency. Brit. Dent J;165:21-22.
7. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesion in bone. J of Am Dent Assoc
1961;87:708-16
8. Saunders MB et al. Reliability of radiographic observation recordedon a performa using inter and intra observer variation:
a preliminary study. Internat Endod j 2000;33:173-85 9. Auer LM, Van V. Intraoperative Ultrasound imaging in Neurosurgery. 1990 Berlin Springer Verlag. 1-11
10. Cotti E et al. A new technique for he study of periapical bone lesion: ultrasound real time imaging. Internat. Endod
J, 2002;35:148-152
11. Srinivasan B. Textbook of Oral and Maxillofacial Surgery.2nd ed,2004: 274-276 |