INTRODUCTION
The association between tobacco and its products represents a significant public health problem. Most epidemiological studies indicate that smoking is directly related to incidence & prevalence of a variety of medical problems including pulmonary, cardiovascular, gastrointestinal disease, low birth weight and cancer. Numerous studies have also demonstrated role of tobacco use on the incidence, prevalence, severity of pocket depth, attachment and alveolar bone loss. Smoking plays a significant role in the development of refractory periodontitis. Smokers have also reported to have poorer success rate with scaling and curettage. Smokers have increased levels of salivary antibodies (IgA) and serum IgG antibodies to P intermedia and F Nucleatum. In addition smokers appear to have depressed number of helper lymphocytes which are important components of the immune systems.
In order for the host to efficiently deal with bacterial infection, fully functioned neutrophils are required. Tobacco smoke can have deleterious effects on neutrophil functions for e.g. it can impair chemotaxis and phagocytosis. The nicotine in tobacco smokers is only one of over 2000 potentially toxic substances. Besides this there are many more components in tobacco smoke which could directly damage the normal cells of the periodontium. These deleterious effects can greatly affect the reparative and regenerative potential of the periodontium in tobacco users.
Another aspect of tobacco and its related products relates to their potential abilities to reduce gingival blood flows besides the direct damage to the periodontal tissues.
MATERIALS AND METHOD
20-55 years males from Mumbai city with the habit of cigarette/bidi smoking participated in this study. For assessment of tobacco disease and periodontal disease the sample were categorised into following groups: Age groups: 20-25yrs,26-35yrs,36-45yrs and 46-55yrs Frequency : average<5units/day,6-10units/day,11-20units/day ,>20units/day. Duration of smoking: <2yrs, 3-5yrs, 6-10yrs and >10yrs.
Individuals currently smoking at least 1 cigarette/bidi were considered as smokers. Individuals smoking one cigarette/bidi in 3 days were considered as occasional smokers. Smoking category included use of either cigarette or bidi or both. Both the forms are most popular in Mumbai reason being cost effective and easy availability. To eliminate bias 26 individuals with systemic problems like diabetes mellitus and heart disease were eliminated.47 individuals who were in a habit of both smokeless form of tobacco consumption and smoking were excluded.
Intraoral examination was conducted by a single examiner, using mouth mirror and WHO probe (CPI).The following scores on 10 index teeth recommended by WHO were recorded:
0- Healthy
1- Bleeding
2- Calculus
3- Pocket of 4-5mm
4- Pocket of 6mm
RESULTS
Cigarette/Bidi smoking had a significant impact on rate of plaque accumulation and hence the severity of periodontal disease. The risk of periodontal disease increases as the duration and frequency of smoking increases.
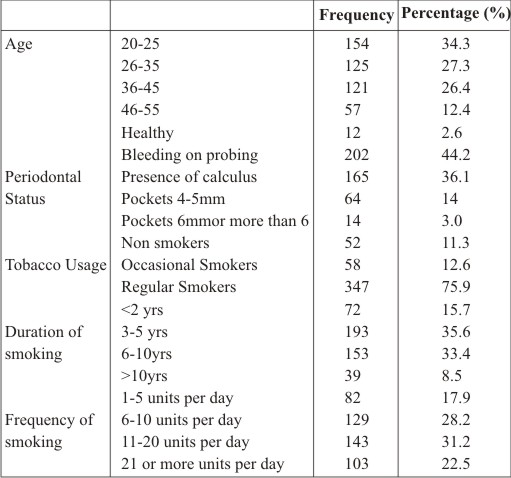 | Table 1-Background and general sample characteristics
 |
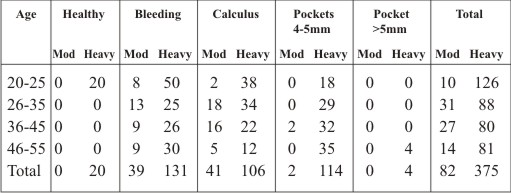 | Sample distribution based on frequency of tobacco consumption in accordance with CPI scores in different age groups
|
Table 1 illustrates the general characteristics of the sample. The youngest and the oldest age groups constituted for a major and minor proportion of the final sample size with 34.3% and 12.4% respectively. There were few subjects (8.5%) who were smoking since 20 years.
Table 2 demonstrates sample distribution based on frequency of smoking in accordance with CPI scores in different age groups
DISCUSSION:
Majority of population studies undertaken in India the sample belongs to low socio economic level. These patients have poor or no access to formal oral health care services. Ironically 78% of the individuals mentioned that they had never been to a dentist. This study also revealed poor oral hygiene habits in the subjects, since most of them restricted to finger with tooth powder and
neem sticks to clean their teeth. The association between the age of the subjects and their periodontal status was evident. Studies have demonstrated a relationship between the prevalence of moderate to severe periodontal disease and the number of cigarettes smoked per day, and the number of years that the patient has smoked. In the present study also long time and heavy smokers were more liable for presenting periodontal pockets.
There is a significant impact of smoking on the severity of periodontal diseases. Also the risk of periodontal pockets increased as the duration and frequency of smoking.
CONCLUSION
The profession of dentistry makes us deal with people addicted to tobacco every day. Different people have different reasons for being enslaved to this habit. Illiterate workers generally are habituated to gutka or paan whereas highly educated corporate workers use smoking as stress buster or fashion symbol. Setting up a clinical practice where some time is allotted for the tobacco deaddiction counselling can not only have a positive impact on society but also aid in maintaining a strong patient dentist relationship.
REFERENCES:
1 Barnstorm J, Preber H. Tobacco use as a risk factor. Jperiodontol 1994; 65: 545-50. Braz J Oral Sci. 7(27):1641-1647 Tobacco as risk factor for periodontal disease in green marble mine laborers of Rajasthan, India164
2. Grossi SG, Zambon JJ, Ho AW, Koch G, Dunford RG, Machtei EE, et al. Assessment of risk for periodontal disease. I. Risk indicators for attachment loss. J Periodontol. 1994; 65: 260-7.
3. Grossi SG, Genco RJ, Machtei EE, Ho AW, Koch G, Dunford R, et al. Assessment of risk for periodontal disease. II. Risk indicators for alveolar bone loss. J Periodontol. 1995; 66: 23-9.
4.Clarke NG, Hirsch RS. Personal risk factors for generalized periodontitis. J Clin Periodontol. 1995; 22: 136-45.
5. Mandel I. Smoke signals: an alert for oral diseases. J Am DentAssoc. 1994; 125: 872-8.
6. Oral health surveys: basic methods. World Health Organization.4th ed. Geneva: WHO; 1997.
7. Peter S. Essentials of preventive and community dentistry.1.ed. Arya (Medi). 2000: 370-415.
8. Johnson GK, Hill M. Cigarette smoking and the periodontal patient. J Periodontol. 2004; 75: 196-209.
9. Newman, Takei, Klokkevold, Carranza. Clinical periodontology. In: John Novak M, Karen F Novak. Smoking and periodontal disease. Elsevier; 2007. p.251-8.
10. Mendis S. Tobacco use in a rural community in Sri Lanka.Ceylon Med J. 1988; 33: 23-6.
11. Ojima M, Hanioka T, Tanaka K, Inoshita E, Aoyama H. Relationship between smoking status and periodontal conditions: findings from national databases in Japan. J Periodont Res. 2006; 41: 573-9.
12. Haber J, Wattles J, Crowley M, Mandell R, Joshipura K, Kent RL. Evidence for cigarette smoking as a major risk factor for periodontitis. J Periodontol. 1993; 64: 16-23.
13. Alpagot T, Wolff LF, Smith QT, Tran SD. Risk indicators for periodontal disease in a racially diverse population. J Clin Periodontol. 1996; 23: 982-8.
14. Haber J, Kent RL. Cigarette smoking in periodontal practice.J Periodontol. 1992; 63: 100-6.
15. Krall EA, Dawson-Hughes B, Garvey AJ, Garcia RI. Smoking, smoking cessation and tooth loss. J Dent Res. 1997; 76: 1653-9. |